

Risk Factors and Temporal Trends of Complications Associated With Transvenous Implantable Cardiac Defibrillator Leads
- PMID: 29748177
- PMCID: PMC6015312
- DOI: 10.1161/JAHA.117.007691
Risk Factors and Temporal Trends of Complications Associated With Transvenous Implantable Cardiac Defibrillator Leads
Abstract
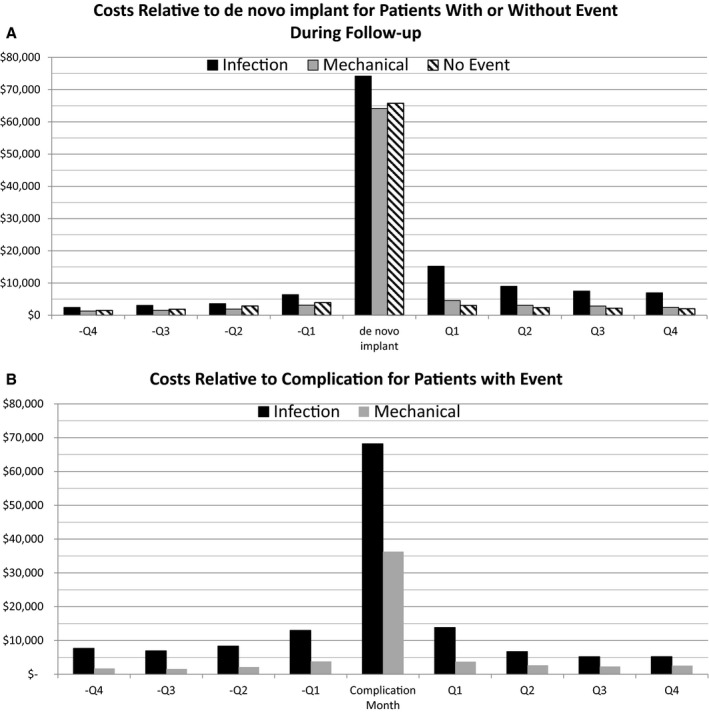
Background: The transvenous implantable cardioverter-defibrillator (ICD) lead is the most common source of complications in a traditional ICD system. This investigation aims to determine the incidence, predictors, and costs associated with these complications using a large insurance database.
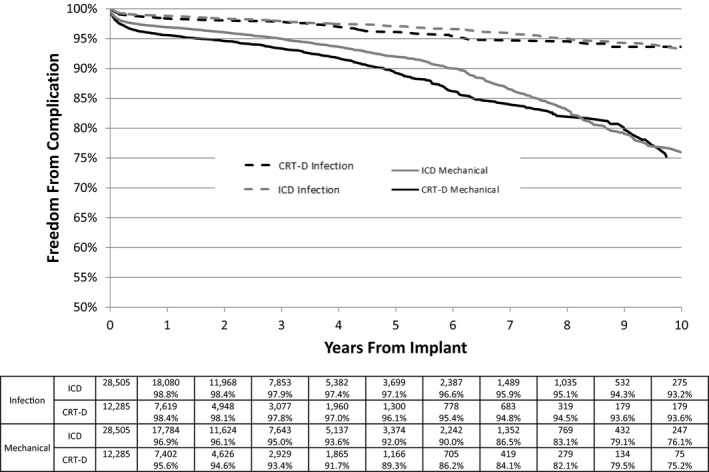
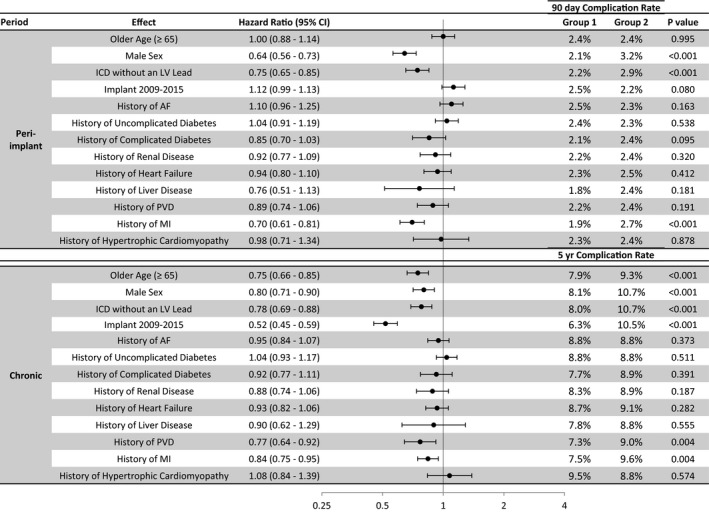
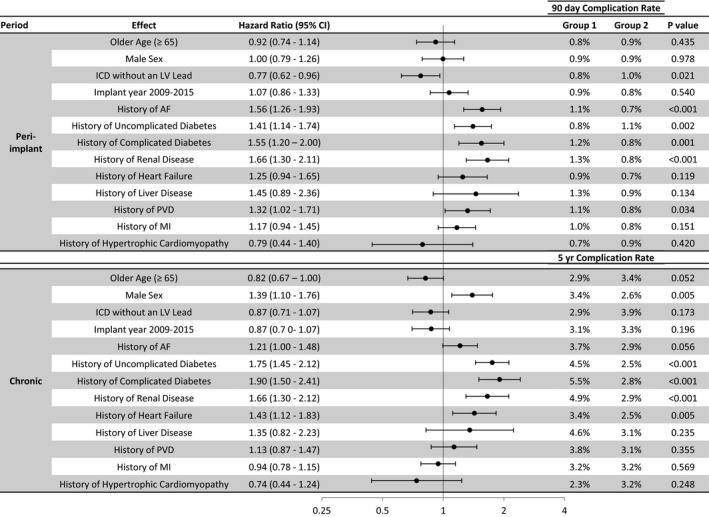
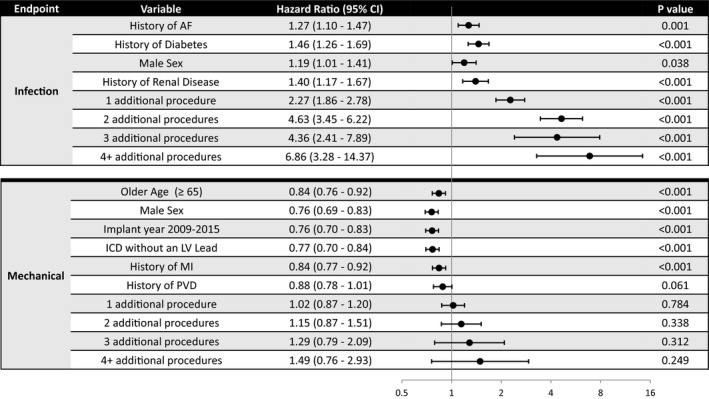
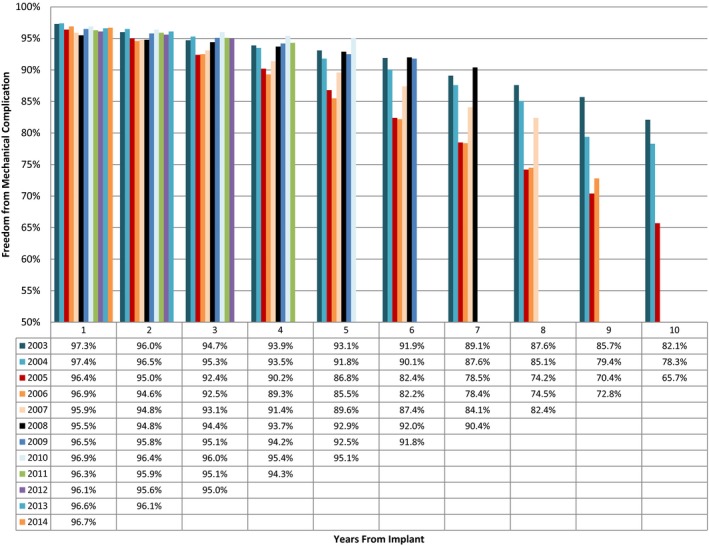
Methods and results: Data from the OptumLabs™ Data Warehouse, which include diagnosis, physician and procedure codes, and claims from patient hospitalizations, were analyzed. Patients with a de novo ICD or cardiac resynchronization therapy defibrillator implanted from January 1, 2003, through June 30, 2015, were included; those who did not have continuous coverage beginning 1 year before implantation were excluded, resulting in 40 837 patients followed up over an average of 2.3±2.1 years. Patients were followed up until they had the procedure or their last active date in the database. Of 20 580 device procedures, 2165 (5.3%) and 771 (1.9%) had mechanical and infectious complications, respectively. The 5-year rate of freedom from mechanical complication was 92.0% and 89.3% for ICDs and cardiac resynchronization therapy defibrillators, respectively. Infectious complications were more likely in patients with a history of atrial fibrillation, diabetes mellitus, and renal disease, and the risk increased with subsequent device procedures. Younger age, female sex, lack of comorbidities, and implantations between 2003 and 2008 were associated with more mechanical complications.
Conclusions: Incidence of mechanical and infectious complications of transvenous ICD leads over long-term follow-up is much higher in the real world than in clinical studies. In our study cohort, 1 of 4 transvenous ICD leads had mechanical complications when followed up to 10 years. The high rate of reintervention leads to additional complications.
Keywords: complication; implantable cardioverter‐defibrillator; infection.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Moss AJ, Hall WJ, Cannom DS, Daubert JP, Higgins SL, Klein H, Levine JH, Saksena S, Waldo AL, Wilber D, Brown MW, Heo M. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. N Engl J Med. 1996;335:1933–1940. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, Daubert JP, Higgins SL, Brown MW, Andrews ML; Multicenter Automatic Defibrillator Implantation Trial II Investigators . Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–883. - PubMed
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, McNulty SE, Clapp‐Channing N, Davidson‐Ray LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH. Amiodarone or an implantable cardioverter—defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–237. - PubMed
-
- Kremers MS, Hammill SC, Berul CI, Koutras C, Curtis JS, Wang Y, Beachy J, Blum Meisnere L, Conyers DM, Reynolds MR, Heidenreich PA, Al‐Khatib SM, Pina IL, Blake K, Norine Walsh M, Wilkoff BL, Shalaby A, Masoudi FA, Rumsfeld J. The National ICD Registry Report: version 2.1 including leads and pediatrics for years 2010 and 2011. Heart Rhythm. 2013;10:e59–e65. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
