

The gut-liver axis and the intersection with the microbiome
- PMID: 29748586
- PMCID: PMC6319369
- DOI: 10.1038/s41575-018-0011-z
The gut-liver axis and the intersection with the microbiome
Erratum in
-
Publisher Correction: The gut-liver axis and the intersection with the microbiome.Nat Rev Gastroenterol Hepatol. 2018 Dec;15(12):785. doi: 10.1038/s41575-018-0031-8. Nat Rev Gastroenterol Hepatol. 2018. PMID: 29785003 Free PMC article.
Abstract
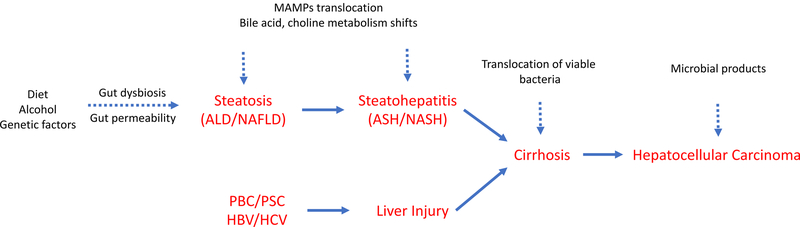
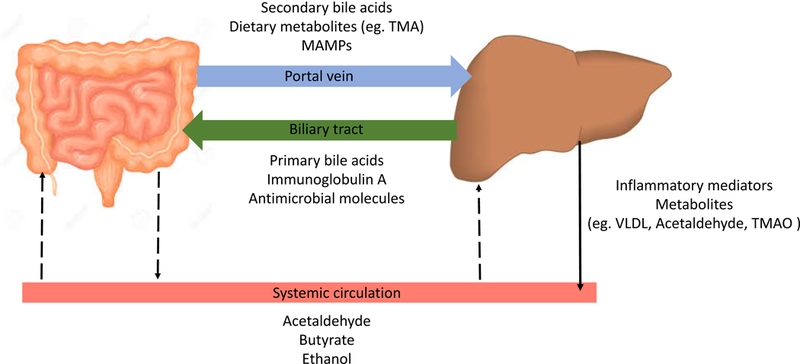
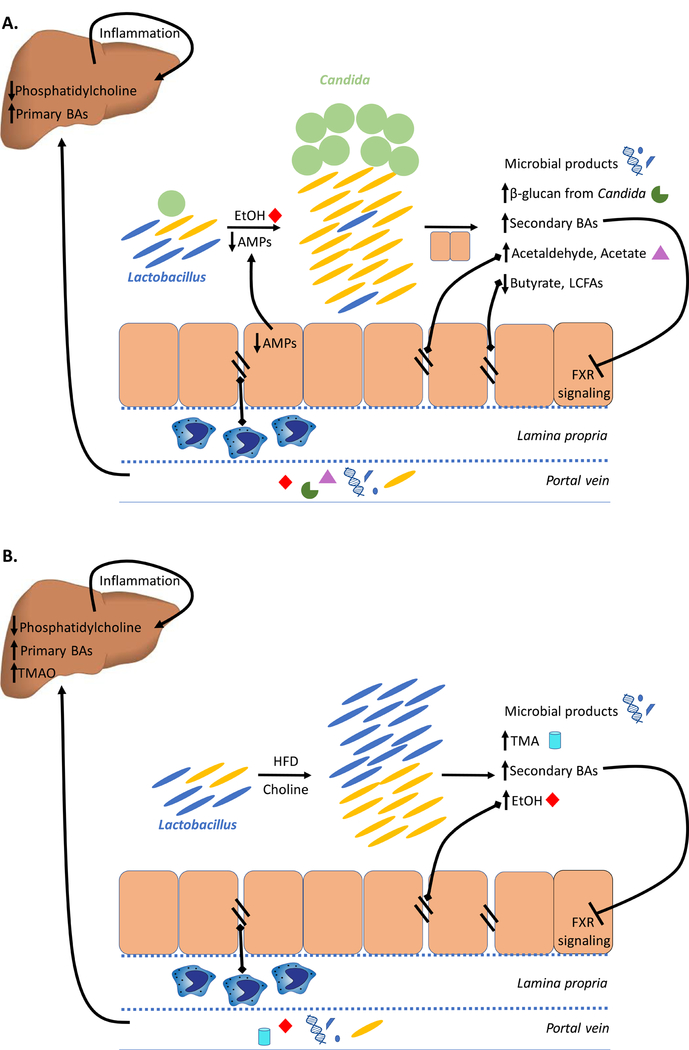
In the past decade, an exciting realization has been that diverse liver diseases - ranging from nonalcoholic steatohepatitis, alcoholic steatohepatitis and cirrhosis to hepatocellular carcinoma - fall along a spectrum. Work on the biology of the gut-liver axis has assisted in understanding the basic biology of both alcoholic fatty liver disease and nonalcoholic fatty liver disease (NAFLD). Of immense importance is the advancement in understanding the role of the microbiome, driven by high-throughput DNA sequencing and improved computational techniques that enable the complexity of the microbiome to be interrogated, together with improved experimental designs. Here, we review gut-liver communications in liver disease, exploring the molecular, genetic and microbiome relationships and discussing prospects for exploiting the microbiome to determine liver disease stage and to predict the effects of pharmaceutical, dietary and other interventions at a population and individual level. Although much work remains to be done in understanding the relationship between the microbiome and liver disease, rapid progress towards clinical applications is being made, especially in study designs that complement human intervention studies with mechanistic work in mice that have been humanized in multiple respects, including the genetic, immunological and microbiome characteristics of individual patients. These 'avatar mice' could be especially useful for guiding new microbiome-based or microbiome-informed therapies.
Conflict of interest statement
Competing interests
The authors declare no competing interests.
Figures
References
-
- Leclercq S et al. Role of intestinal permeability and inflammation in the biological and behavioral control of alcohol-dependent subjects. Brain. Behav. Immun 26, 911–918 (2012). (role of inflammation in ALD and reversibility on abstinence in humans) - PubMed
-
- Zhu L et al. Characterization of gut microbiomes in nonalcoholic steatohepatitis (NASH) patients: A connection between endogenous alcohol and NASH. Hepatology 57, 601–609 (2013). (elevated ethanol production by gut microbiota in pediatric NASH patients) - PubMed
Publication types
MeSH terms
Grants and funding
- R01 AA020703/AA/NIAAA NIH HHS/United States
- R37 AI043477/AI/NIAID NIH HHS/United States
- P42 ES010337/ES/NIEHS NIH HHS/United States
- U01 AA021856/AA/NIAAA NIH HHS/United States
- U01 AA024726/AA/NIAAA NIH HHS/United States
- R01 DK072237/DK/NIDDK NIH HHS/United States
- R01 CA118165/CA/NCI NIH HHS/United States
- R01 GM041804/GM/NIGMS NIH HHS/United States
- R01 DK106419/DK/NIDDK NIH HHS/United States
- P50 AA011999/AA/NIAAA NIH HHS/United States
- R01 AA015055/AA/NIAAA NIH HHS/United States
- I01 BX002213/BX/BLRD VA/United States
- R01 AI043477/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
