

Myeloid-derived suppressor cells (MDSCs) in patients with solid tumors: considerations for granulocyte colony-stimulating factor treatment
- PMID: 29748897
- PMCID: PMC11028306
- DOI: 10.1007/s00262-018-2166-4
Myeloid-derived suppressor cells (MDSCs) in patients with solid tumors: considerations for granulocyte colony-stimulating factor treatment
Abstract
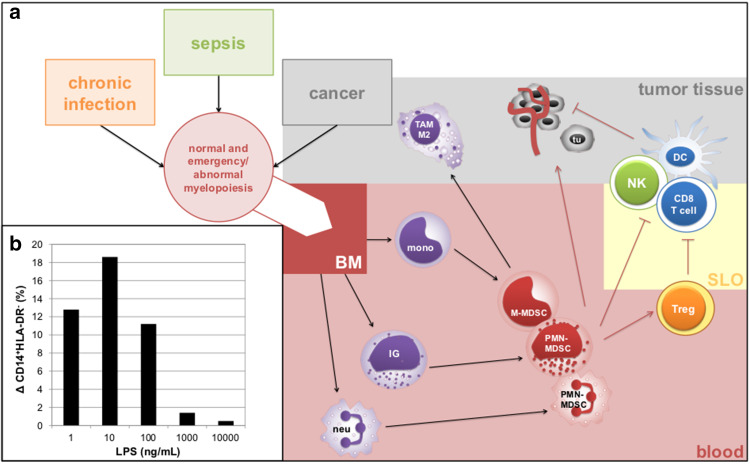
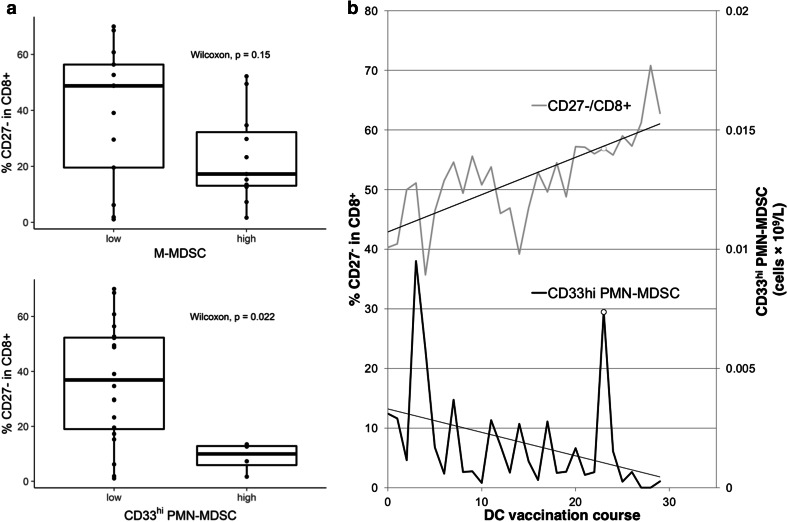
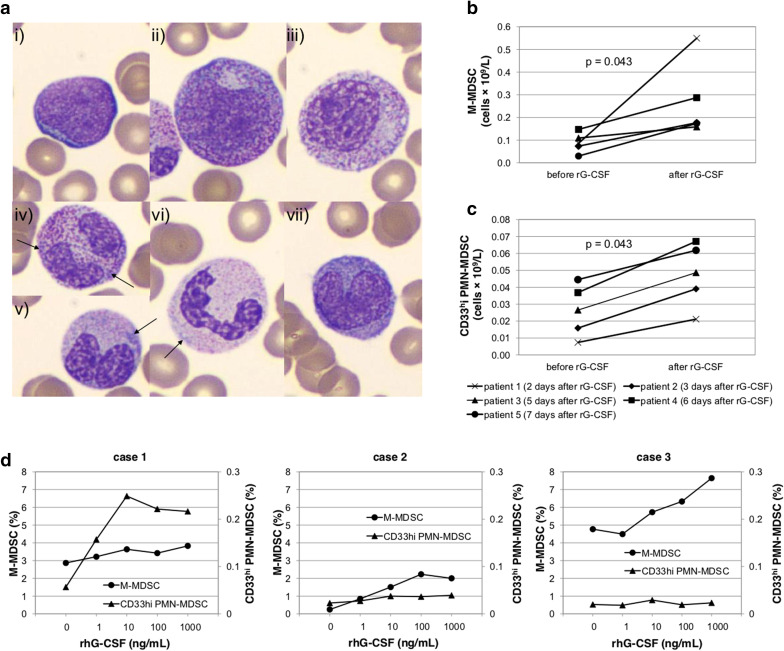
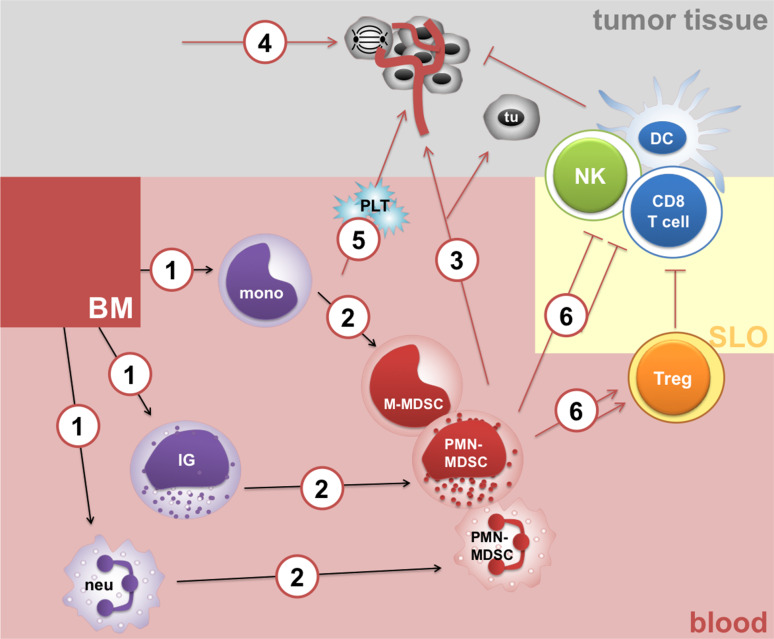
Myeloid-derived suppressor cells (MDSCs) have been shown to contribute to tumor escape from host immune surveillance and to cancer progression by production of tumor-promoting soluble factors. Granulocyte colony-stimulating factor (G-CSF) is a principle cytokine controlling granulocyte number. Recombinant human G-CSF (rhG-CSF) has become the main therapeutic agent for the treatment of neutropenia and prophylaxis of febrile neutropenia in cancer patients. However, we show here that rhG-CSF triggers accumulation of granulocytic and monocytic subsets. Consequently, we discuss the pharmacological use of granulopoiesis stimulating factors not only in the context of febrile neutropenia but also from the perspective of MDSC-dependent and MDSC-independent mechanisms of immunosuppression and cancer angiogenesis.
Keywords: CITIM 2017; Cancer; Granulocyte colony-stimulating factor; Myeloid-derived suppressor cells; Prophylaxis of febrile neutropenia.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
The downregulation of type I IFN signaling in G-MDSCs under tumor conditions promotes their development towards an immunosuppressive phenotype.Cell Death Dis. 2022 Jan 10;13(1):36. doi: 10.1038/s41419-021-04487-w. Cell Death Dis. 2022. PMID: 35013108 Free PMC article.
-
Aerobic Glycolysis Controls Myeloid-Derived Suppressor Cells and Tumor Immunity via a Specific CEBPB Isoform in Triple-Negative Breast Cancer.Cell Metab. 2018 Jul 3;28(1):87-103.e6. doi: 10.1016/j.cmet.2018.04.022. Epub 2018 May 24. Cell Metab. 2018. PMID: 29805099 Free PMC article.
-
Allogeneic Hematopoietic Stem Cell Transplantation Mobilized With Pegylated Granulocyte Colony-Stimulating Factor Ameliorates Severe Acute Graft-Versus-Host Disease Through Enrichment of Monocytic Myeloid-Derived Suppressor Cells in the Graft: A Real World Experience.Front Immunol. 2021 Apr 12;12:621935. doi: 10.3389/fimmu.2021.621935. eCollection 2021. Front Immunol. 2021. PMID: 33912154 Free PMC article.
-
Granulocytic Myeloid-Derived Suppressor Cells as Negative Regulators of Anticancer Immunity.Front Immunol. 2020 Aug 27;11:1963. doi: 10.3389/fimmu.2020.01963. eCollection 2020. Front Immunol. 2020. PMID: 32983128 Free PMC article. Review.
-
The role of colony-stimulating factors and granulocyte transfusion in treatment options for neutropenia in children with cancer.Paediatr Drugs. 2003;5(10):673-84. doi: 10.2165/00148581-200305100-00003. Paediatr Drugs. 2003. PMID: 14510625 Review.
Cited by
-
CD244+ polymorphonuclear myeloid‑derived suppressor cells reflect the status of peritoneal dissemination in a colon cancer mouse model.Oncol Rep. 2021 Jun;45(6):106. doi: 10.3892/or.2021.8057. Epub 2021 Apr 28. Oncol Rep. 2021. PMID: 33907826 Free PMC article.
-
Resistance to Immune Checkpoint Inhibitors Secondary to Myeloid-Derived Suppressor Cells: A New Therapeutic Targeting of Haematological Malignancies.J Clin Med. 2021 Apr 28;10(9):1919. doi: 10.3390/jcm10091919. J Clin Med. 2021. PMID: 33925214 Free PMC article. Review.
-
Pathological and Molecular Features of Glioblastoma and Its Peritumoral Tissue.Cancers (Basel). 2019 Apr 3;11(4):469. doi: 10.3390/cancers11040469. Cancers (Basel). 2019. PMID: 30987226 Free PMC article. Review.
-
Granulocyte colony-stimulating factor has the potential to attenuate the therapeutic efficacy of chemo-immunotherapy for extensive-stage small-cell lung cancer.Int J Clin Oncol. 2024 Oct;29(10):1451-1460. doi: 10.1007/s10147-024-02586-0. Epub 2024 Jul 15. Int J Clin Oncol. 2024. PMID: 39009900
-
Disseminated carcinomatosis of the bone marrow caused by granulocyte colony-stimulating factor: A case report and review of literature.World J Gastrointest Oncol. 2022 Oct 15;14(10):2077-2084. doi: 10.4251/wjgo.v14.i10.2077. World J Gastrointest Oncol. 2022. PMID: 36310701 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
