

Obinutuzumab plus bendamustine in previously untreated patients with CLL: a subgroup analysis of the GREEN study
- PMID: 29749403
- PMCID: PMC6087718
- DOI: 10.1038/s41375-018-0146-5
Obinutuzumab plus bendamustine in previously untreated patients with CLL: a subgroup analysis of the GREEN study
Abstract
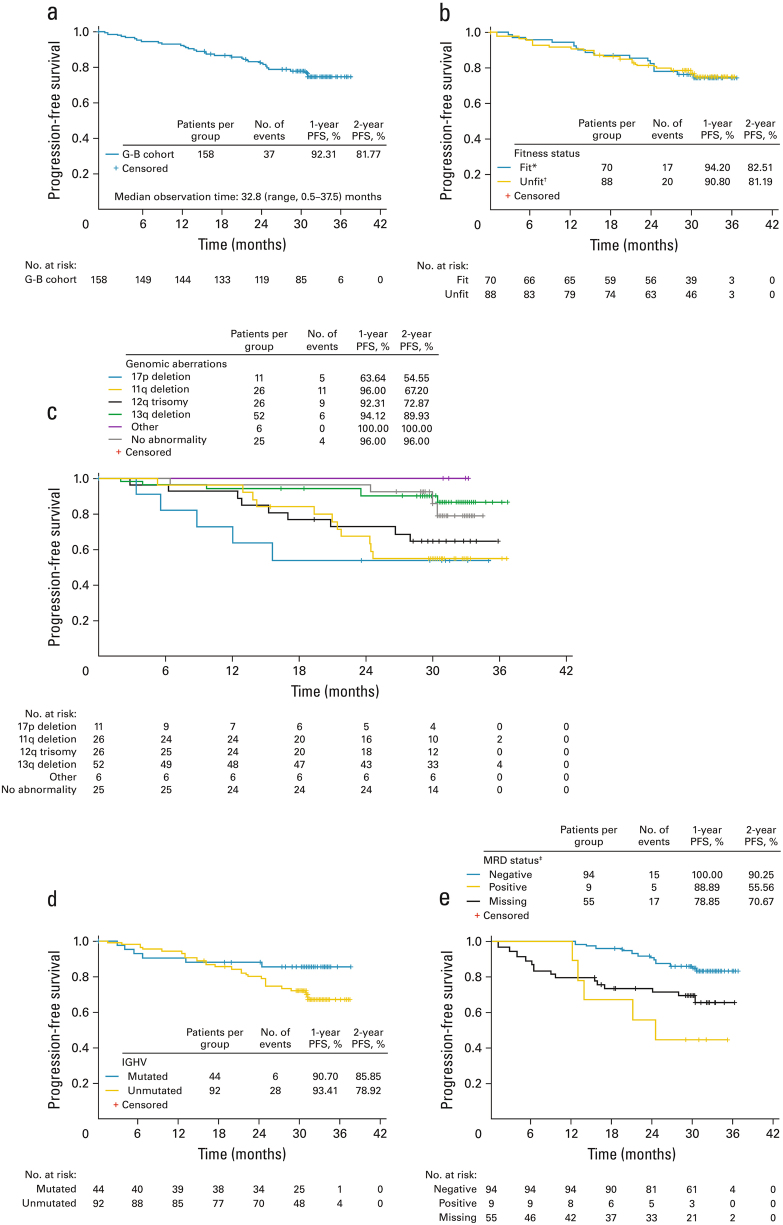
GREEN (NCT01905943) is a non-randomized, open-label phase IIIb study investigating obinutuzumab alone or plus chemotherapy in chronic lymphocytic leukemia (CLL). We report a preplanned subgroup analysis of 158 previously untreated CLL patients receiving obinutuzumab-bendamustine (G-B). Patients received six 28-day cycles (C) of G-B: obinutuzumab day (D)1/D2 of C1 (25 mg D1/975 mg D2), 1000 mg D8 and D15 of C1, and D1 of C2-6; and bendamustine 70/90 mg/m2 D1 and D2 of C1-6. The primary endpoint was safety/tolerability. Grade ≥3 adverse events (AEs) occurred in 82.3% of patients, including neutropenia (49.4%), thrombocytopenia (12.0%) and febrile neutropenia (10.8%). Serious AEs included neutropenia (12.7%), febrile neutropenia (9.5%) and pneumonia (7.6%). Rates of grade ≥3 infections and infusion-related reactions were 20.3% and 17.1%, respectively. Due to tumor lysis syndrome (TLS; 8.2%), including two associated fatalities (one in another study cohort), additional risk-minimization measures were implemented. Overall response rate was 81.0%. After 32.8 months' median observation time, 2-year progression-free survival was 81.8%. Minimal residual disease was undetectable in 59.5% (94/158) and 27.8% (44/158) of patients for blood and bone marrow, respectively. Frontline G-B appears to have manageable toxicity with clinical activity in CLL. Careful TLS risk assessment, pretreatment and monitoring is required.
Conflict of interest statement
SS reports consulting fees, research funding, honoraria and membership of advisory committees from Roche. VL reports speaker’s bureau fees, consulting fees, research funding, honoraria and membership of advisory committees from Roche; speaker’s bureau fees, consulting fees, honoraria and membership of advisory committees from Janssen; speaker’s bureau fees, honoraria and membership of advisory committees from Gilead and GSK; membership of advisory committees for AbbVie; and speaker’s bureau fees from Mundipharma. RF reports speaker’s bureau fees, consulting fees, honoraria and membership of advisory committees from Roche, Janssen, Celgene, AbbVie, Amgen and Novartis. SB reports consulting fees from Roche and AbbVie; research funding from Roche, AbbVie and Celgene; and honoraria from Roche, AbbVie and Beckton Dickinson. WK reports honoraria and participation in advisory boards for Roche and Mundipharma. CR reports research funding and membership of advisory committees from Roche and Celgene. FB reports consulting fees and honoraria from Roche, Novartis, Janssen, AbbVie, Gilead and Mundipharma; and research funding from Roche and Janssen. OI, EM, ET and DW report research funding from Roche. EG, LL, T Moore, T Morris and SR report employment from Roche.
Figures
References
-
- Eichhorst B, Fink AM, Bahlo J, Busch R, Kovacs G, Maurer C, et al. First-line chemoimmunotherapy with bendamustine and rituximab versus fludarabine, cyclophosphamide, and rituximab in patients with advanced chronic lymphocytic leukaemia (CLL10): an international, open-label, randomised, phase 3, non-inferiority trial. Lancet Oncol. 2016;17:928–42. doi: 10.1016/S1470-2045(16)30051-1. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
