

Light-sheet microscopy for slide-free non-destructive pathology of large clinical specimens
- PMID: 29750130
- PMCID: PMC5940348
- DOI: 10.1038/s41551-017-0084
Light-sheet microscopy for slide-free non-destructive pathology of large clinical specimens
Abstract
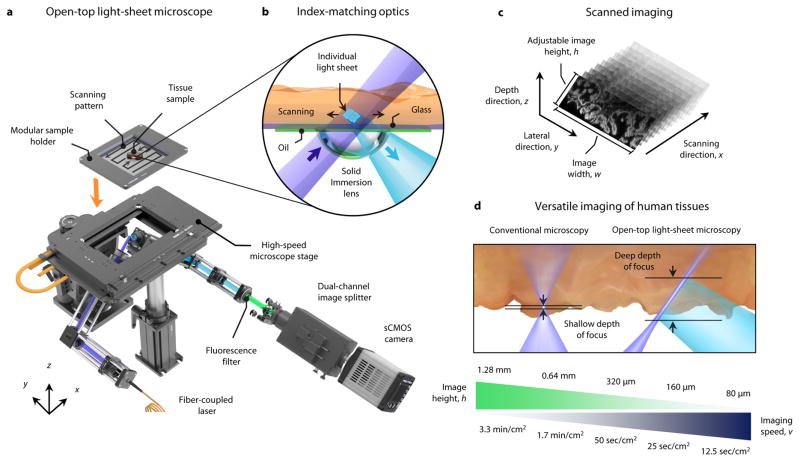
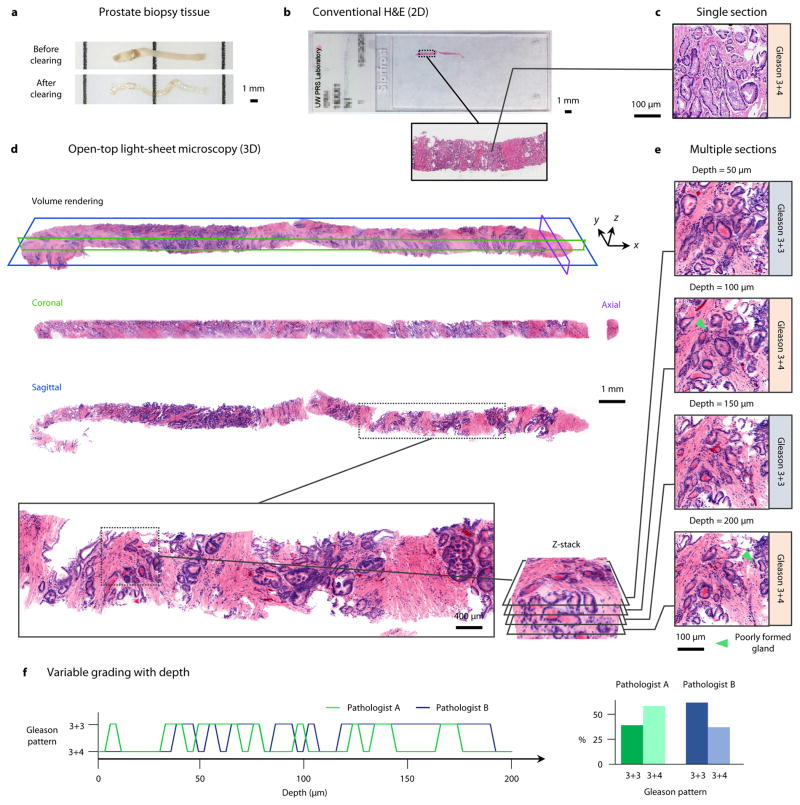
For the 1.7 million patients per year in the U.S. who receive a new cancer diagnosis, treatment decisions are largely made after a histopathology exam. Unfortunately, the gold standard of slide-based microscopic pathology suffers from high inter-observer variability and limited prognostic value due to sampling limitations and the inability to visualize tissue structures and molecular targets in their native 3D context. Here, we show that an open-top light-sheet microscope optimized for non-destructive slide-free pathology of clinical specimens enables the rapid imaging of intact tissues at high resolution over large 2D and 3D fields of view, with the same level of detail as traditional pathology. We demonstrate the utility of this technology for various applications: wide-area surface microscopy to triage surgical specimens (with ~200 μm surface irregularities), rapid intraoperative assessment of tumour-margin surfaces (12.5 sec/cm2), and volumetric assessment of optically cleared core-needle biopsies (1 mm in diameter, 2 cm in length). Light-sheet microscopy can be a versatile tool for both rapid surface microscopy and deep volumetric microscopy of human specimens.
Conflict of interest statement
Competing interests The authors declare no competing financial interests.
Figures


References
-
- Surveillance Research Program, N.C.I. [12-13-2016];Fast Stats: An interactive tool for access to SEER cancer statistics. 2016 Available from: https://seer.cancer.gov/faststats/
-
- Barakat FH, Sulaiman I, Sughayer MA. Reliability of frozen section in breast sentinel lymph node examination. Breast Cancer. 2014;21(5):576–82. - PubMed
-
- McKenney JK, et al. The potential impact of reproducibility of Gleason grading in men with early stage prostate cancer managed by active surveillance: a multi-institutional study. J Urol. 2011;186(2):465–9. - PubMed
-
- Shah RB, et al. Diagnosis of Gleason pattern 5 prostate adenocarcinoma on core needle biopsy: an interobserver reproducibility study among urologic pathologists. Am J Surg Pathol. 2015;39(9):1242–9. - PubMed
-
- Meyer JS, et al. Breast carcinoma malignancy grading by Bloom-Richardson system vs proliferation index: reproducibility of grade and advantages of proliferation index. Mod Pathol. 2005;18(8):1067–78. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
