

Diagnostic accuracy between readers for identifying electrographic seizures in critically ill adults
- PMID: 29750214
- PMCID: PMC5939393
- DOI: 10.1002/epi4.12034
Diagnostic accuracy between readers for identifying electrographic seizures in critically ill adults
Abstract
Objective: Electrographic seizures in critically ill patients are often equivocal. In this study, we sought to determine the diagnostic accuracy of electrographic seizure annotation in adult intensive care units (ICUs) and to identify affecting factors.
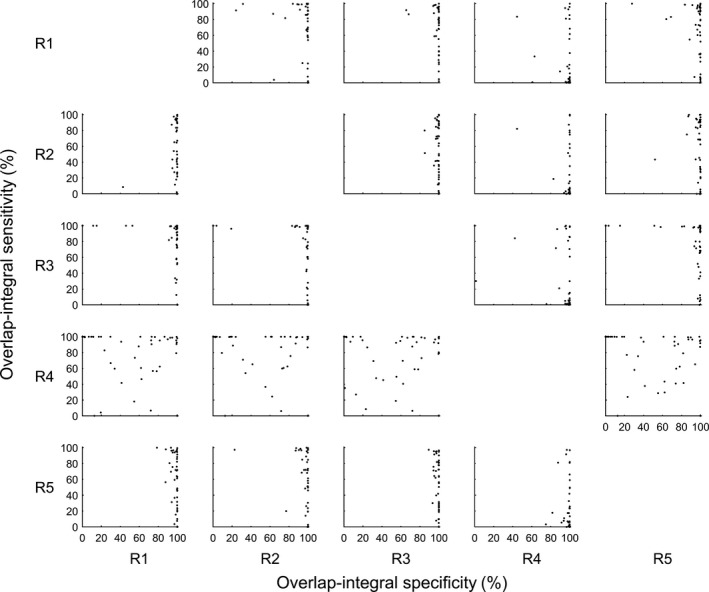
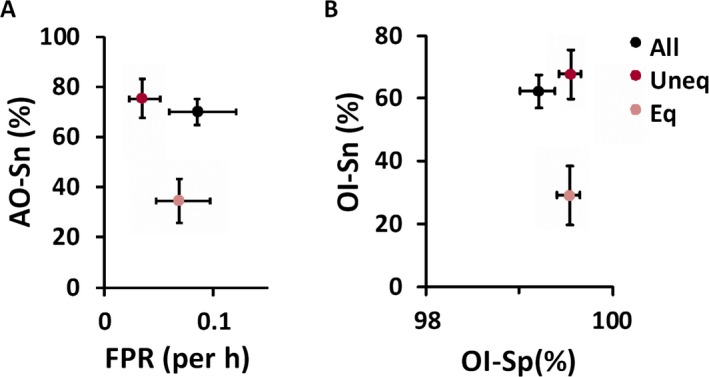
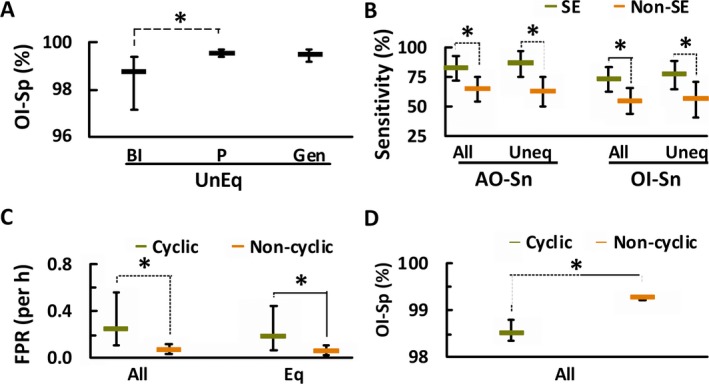
Methods: To investigate diagnostic accuracy, interreader agreement (IRA) measures were derived from 5,769 unequivocal and 6,263 equivocal seizure annotations by five experienced electroencephalogram (EEG) readers after reviewing 74 days of EEGs from 50 adult ICU patients. Factors including seizure equivocality (unequivocal vs. equivocal) and laterality (generalized, partial, or bilaterally independent), cyclicity (cyclic vs. noncyclic), persistency (occurrence of status epilepticus), and patient consciousness level (coma vs. noncoma) were further investigated for their influence on IRA measures.
Results: On average, 70% of seizures marked by a reference reader overlapped, at least in part, with those marked by a test reader (any-overlap sensitivity, AO-Sn). Agreed seizure duration between reader pairs (overlap-integral sensitivity, OI-Sn) was 62%, while agreed nonseizure duration (overlap-integral specificity, OI-Sp) was 99%. A test reader would annotate one additional seizure not overlapping with a reference reader's annotation in every 11.7 h of EEG, that is, the false-positive rate (FPR) was 0.0854/h. Classifying seizure patterns into unequivocal and equivocal improved specificity and FPR (unequivocal patterns) but compromised sensitivity only for equivocal patterns. Sensitivity of all and unequivocal annotations was higher for patients with status epilepticus. Specificity was higher for partial than for bilaterally independent unequivocal seizure patterns, and lower for cyclic all seizure patterns.
Significance: Diagnosing electrographic seizures in critically ill adults is highly specific and moderately sensitive. Improved criteria for diagnosing electrographic seizures in the ICU are needed.
Keywords: Continuous EEG monitoring; Critical care; Epilepsy; Equivocal seizures; Interreader agreement.
Figures

References
-
- Jordan KG. Continuous EEG monitoring in the neuroscience intensive care unit and emergency department. J Clin Neurophysiol 1999;16:14–39. - PubMed
-
- Claassen J, Mayer SA, Kowalski RG, et al. Detection of electrographic seizures with continuous EEG monitoring in critically ill patients. Neurology 2004;62:1743–1748. - PubMed
-
- Kurtz P, Gaspard N, Wahl AS, et al. Continuous electroencephalography in a surgical intensive care unit. Intensive Care Med 2014;40:228–234. - PubMed
-
- Oddo M, Carrera E, Claassen J, et al. Continuous electroencephalography in the medical intensive care unit. Crit Care Med 2009;37:2051–2056. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
