

A population-based cost-effectiveness study of early genetic testing in severe epilepsies of infancy
- PMID: 29750358
- PMCID: PMC5990455
- DOI: 10.1111/epi.14087
A population-based cost-effectiveness study of early genetic testing in severe epilepsies of infancy
Abstract
Objective: The severe epilepsies of infancy (SEI) are a devastating group of disorders that pose a major care and economic burden on society; early diagnosis is critical for optimal management. This study sought to determine the incidence and etiologies of SEI, and model the yield and cost-effectiveness of early genetic testing.
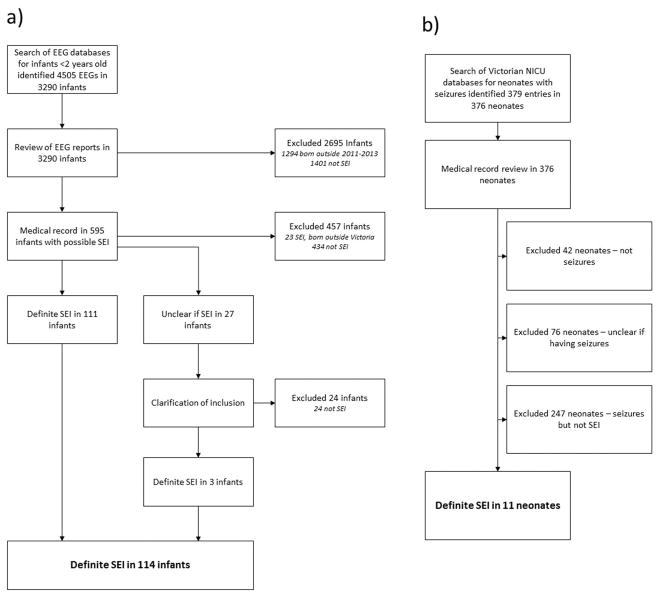
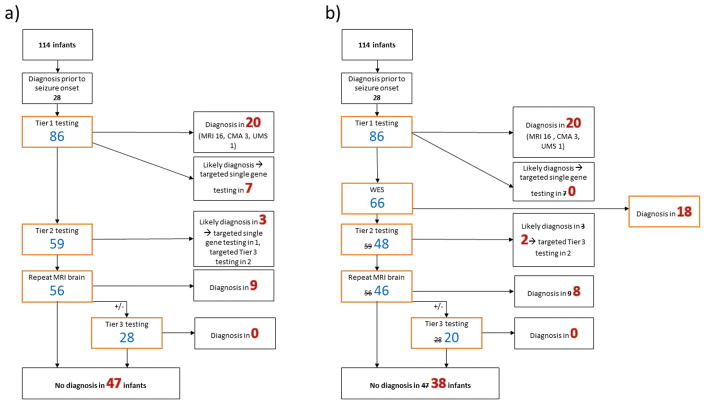
Methods: A population-based study was undertaken of the incidence, etiologies, and cost-effectiveness of a whole exome sequencing-based gene panel (targeted WES) in infants with SEI born during 2011-2013, identified through electroencephalography (EEG) and neonatal databases. SEI was defined as seizure onset before age 18 months, frequent seizures, epileptiform EEG, and failure of ≥2 antiepileptic drugs. Medical records, investigations, MRIs, and EEGs were analyzed, and genetic testing was performed if no etiology was identified. Economic modeling was performed to determine yield and cost-effectiveness of investigation of infants with unknown etiology at epilepsy onset, incorporating targeted WES at different stages of the diagnostic pathway.
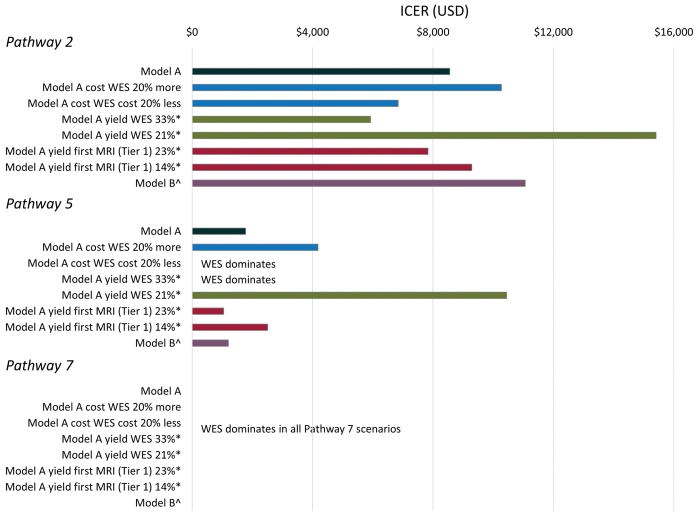
Results: Of 114 infants with SEI (incidence = 54/100 000 live births/y), the etiology was determined in 76 (67%): acquired brain injuries (n = 14), focal cortical dysplasias (n = 14), other brain malformations (n = 17), channelopathies (n = 11), chromosomal (n = 9), metabolic (n = 6), and other genetic (n = 5) disorders. Modeling showed that incorporating targeted WES increased diagnostic yield compared to investigation without targeted WES (48/86 vs 39/86). Early targeted WES had lower total cost ($677 081 U.S. dollars [USD] vs $738 136 USD) than late targeted WES. A pathway with early targeted WES and limited metabolic testing yielded 7 additional diagnoses compared to investigation without targeted WES (46/86 vs 39/86), with lower total cost ($455 597 USD vs $661 103 USD), lower cost per diagnosis ($9904 USD vs $16 951 USD), and a dominant cost-effectiveness ratio.
Significance: Severe epilepsies occur in 1 in 2000 infants, with the etiology identified in two-thirds, most commonly malformative. Early use of targeted WES yields more diagnoses at lower cost. Early genetic diagnosis will enable timely administration of precision medicines, once developed, with the potential to improve long-term outcome.
Keywords: epilepsy; etiology; genomic; health economic; incidence; infancy.
Wiley Periodicals, Inc. © 2018 International League Against Epilepsy.
Conflict of interest statement
Dr Howell was supported by the Gustav Nossal National Health and Medical Research Council (NHMRC) Postgraduate Scholarship and the Clifford PhD Scholarship. Dr Mefford is support by National Institutes of Health (NINDS R01 NS069605). Prof Scheffer is supported by a NHMRC Program Grant and Practitioner Fellowship. None of the authors has any conflicts of interest to disclose.
Figures
References
-
- Organisation WH. Neurological disorders: Public Health Challenges. 2006.
-
- Berg AT, Berkovic SF, Brodie MJ, et al. Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAE Commission on Classification and Terminology, 2005–2009. Epilepsia. 2010;51:676–85. - PubMed
-
- McTague A, Howell KB, Cross JH, Kurian MA, Scheffer IE. The genetic landscape of the epileptic encephalopathies of infancy and childhood. Lancet Neurol. 2016;15:304–16. - PubMed
-
- Bureau M, Thomas P, Genton P. Epileptic syndromes in infancy, childhood and adolescence. p. 682. Fifth edition with video sequences. ed:1 online resource.
-
- Wilmshurst JM, Gaillard WD, Vinayan KP, et al. Summary of recommendations for the management of infantile seizures: Task Force Report for the ILAE Commission of Pediatrics. Epilepsia. 2015;56:1185–97. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Other Literature Sources