

Disparities in Initiation of Direct-Acting Antiviral Agents for Hepatitis C Virus Infection in an Insured Population
- PMID: 29750893
- PMCID: PMC6055302
- DOI: 10.1177/0033354918772059
Disparities in Initiation of Direct-Acting Antiviral Agents for Hepatitis C Virus Infection in an Insured Population
Abstract
Objectives: The cost of direct-acting antiviral agents (DAAs) for hepatitis C virus (HCV) infection may contribute to treatment disparities. However, few data exist on factors associated with DAA initiation.
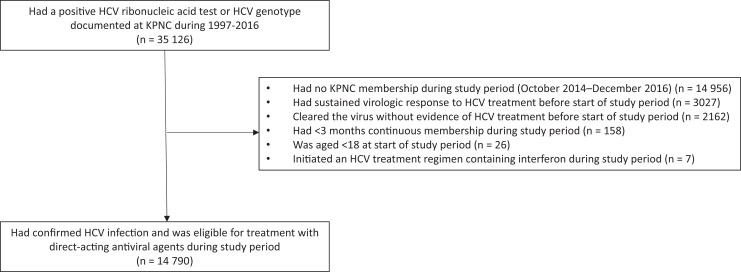
Methods: We conducted a retrospective cohort study of HCV-infected Kaiser Permanente Northern California members aged ≥18 during October 2014 to December 2016, using Poisson regression models to evaluate demographic, behavioral, and clinical factors associated with DAA initiation.
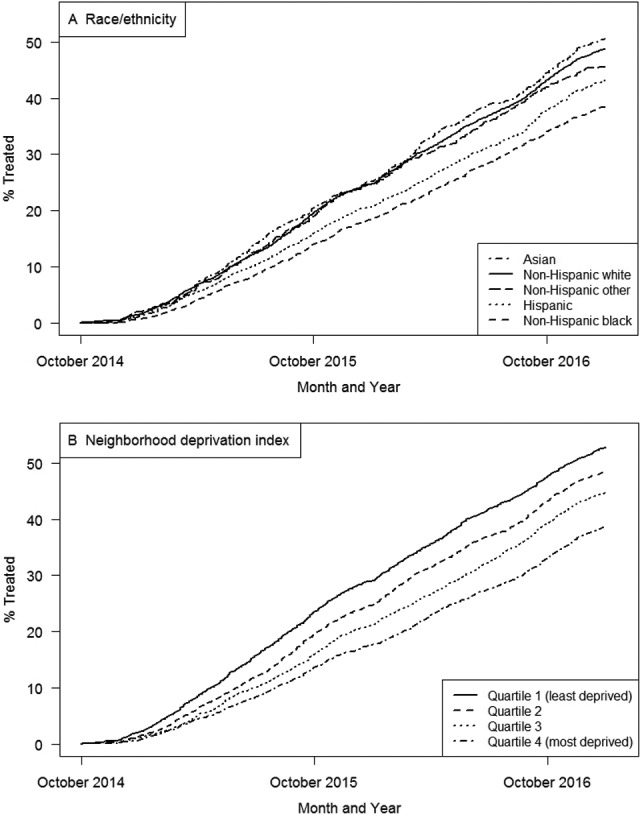
Results: Of 14 790 HCV-infected patients aged ≥18 (median age, 60; interquartile range, 53-64), 6148 (42%) initiated DAAs. DAA initiation was less likely among patients who were non-Hispanic black (adjusted rate ratio [aRR] = 0.7; 95% confidence interval [CI], 0.7-0.8), Hispanic (aRR = 0.8; 95% CI, 0.7-0.9), and of other minority races/ethnicities (aRR = 0.9; 95% CI, 0.8-1.0) than among non-Hispanic white people and among those with lowest compared with highest neighborhood deprivation index (ie, a marker of socioeconomic status) (aRR = 0.8; 95% CI, 0.7-0.8). Having maximum annual out-of-pocket health care costs >$3000 compared with ≤$3000 (aRR = 0.9; 95% CI, 0.8-0.9) and having Medicare (aRR = 0.8; 95% CI, 0.8-0.9) or Medicaid (aRR = 0.7; 95% CI, 0.6-0.8) compared with private health insurance were associated with a lower likelihood of DAA initiation. Behavioral factors (eg, drug abuse diagnoses, alcohol use, and smoking) were also significantly associated with a lower likelihood of DAA initiation (all P < .001). Clinical factors associated with a higher likelihood of DAA initiation were advanced liver fibrosis, HCV genotype 1, previous HCV treatment (all P < .001), and HIV infection ( P = .007).
Conclusions: Racial/ethnic and socioeconomic disparities exist in DAA initiation. Substance use may also influence patient or provider decision making about DAA initiation. Strategies are needed to ensure equitable access to DAAs, even in insured populations.
Keywords: health care delivery; hepatitis; racial disparities; substance abuse; treatment.
Conflict of interest statement
Figures
References
-
- Centers for Disease Control and Prevention. Disease burden from viral hepatitis A, B, and C in the United States. 2016. http://www.cdc.gov/hepatitis/HCV/StatisticsHCV.htm. Accessed November 6, 2017.
-
- Chak E, Talal AH, Sherman KE, Schiff ER, Saab S. Hepatitis C virus infection in USA: an estimate of true prevalence. Liver Int. 2011;31(8):1090–1101. - PubMed
-
- Mahajan R, Xing J, Liu SJ, et al. Mortality among persons in care with hepatitis C virus infection: the Chronic Hepatitis Cohort Study (CHeCS), 2006-2010 [published correction appears in Clin Infect Dis. 2014;58(12):1792]. Clin Infect Dis. 2014;58(8):1055–1061. - PubMed
-
- Mehta SH, Lucas GM, Mirel LB, et al. Limited effectiveness of antiviral treatment for hepatitis C in an urban HIV clinic. AIDS. 2006;20(18):2361–2369. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
