

The Gender Impact on Morphogenetic Variability in Coronary Artery Disease: A Preliminary Study
- PMID: 29751567
- PMCID: PMC5977142
- DOI: 10.3390/jcm7050103
The Gender Impact on Morphogenetic Variability in Coronary Artery Disease: A Preliminary Study
Abstract
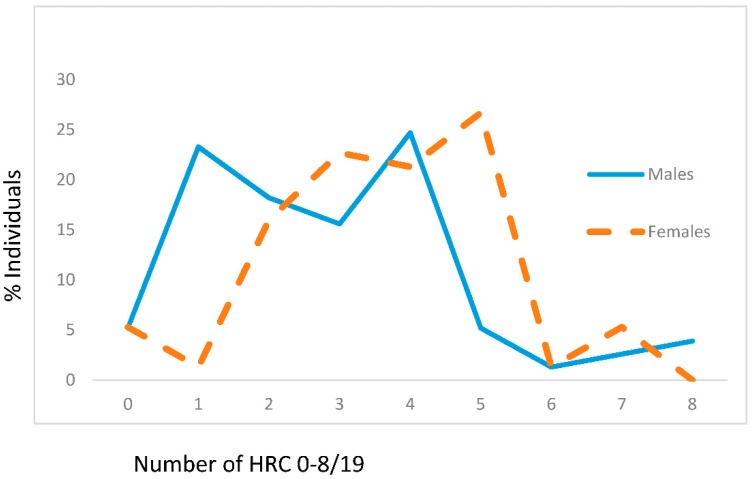
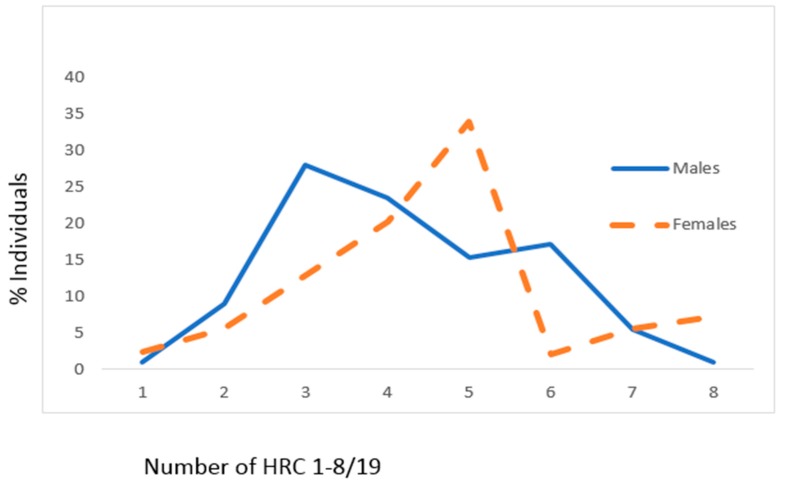
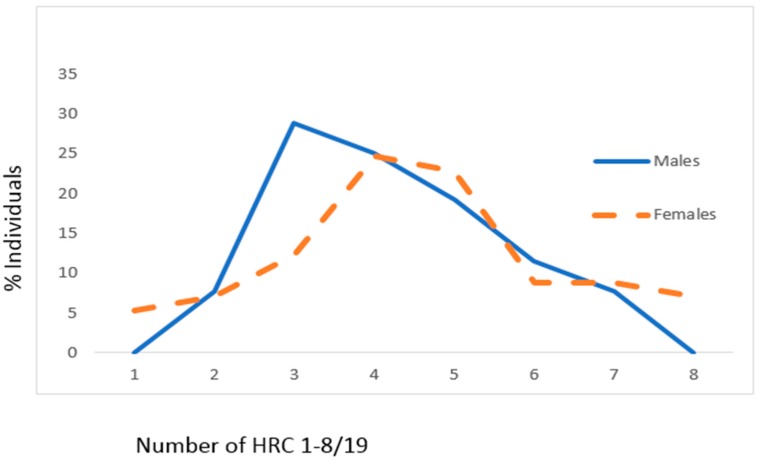
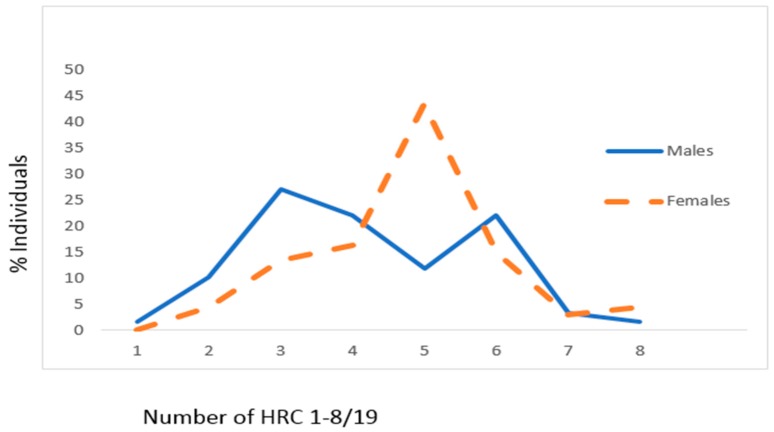
We analyzed morphogenetic variability and degree of genetic homozygosity in male and female individuals with coronary artery disease (CAD) versus unaffected controls. We have tested 235 CAD patients; 109 were diagnosed also with diabetes mellitus (DM) and 126 with hypertension (HTN). We additionally evaluated 152 healthy individuals without manifested CAD. For the evaluation of the degree of recessive homozygosity, we have performed the homozygously recessive characteristics (HRC) test and tested 19 HRCs. In controls, the frequency of HRC for males was 2.88 ± 1.89, while for females, it was 3.65 ± 1.60. In the CAD group, the frequency of HRC for males was 4.21 ± 1.47, while for females, it was 4.73 ± 1.60. There is significant difference in HRC frequencies between controls and CAD separately for males (p < 0.001) and females (p < 0.001). The same applies between controls and CAD with DM (males: p < 0.001 and females: p = 0.004), and controls and CAD with HTN (males: p < 0.001 and females: p < 0.001). There is no significant difference in HRC frequencies between the group of CAD with DM and the group of CAD with HTN (males: p = 0.952 and females: p = 0.529). Our findings point to the increased degree of recessive homozygosity and decreased variability in both genders of CAD patients versus controls, indicating the potential genetic predisposition for CAD.
Keywords: coronary artery disease; gender; homozygous recessive characteristics; variability.
Conflict of interest statement
Authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
