

Validating the use of veterans affairs tobacco health factors for assessing change in smoking status: accuracy, availability, and approach
- PMID: 29751746
- PMCID: PMC5948734
- DOI: 10.1186/s12874-018-0501-2
Validating the use of veterans affairs tobacco health factors for assessing change in smoking status: accuracy, availability, and approach
Abstract
Background: Accurate smoking status is key for research purposes, but can be costly and difficult to measure. Within the Veteran's Health Administration (VA), smoking status is recorded as part of routine care as "health factors" (HF)-fields that researchers can query through the electronic health record (EHR). Many researchers are interested in using these fields to track changes in smoking status over time, however the validity of this measure for assessing change is unknown. The primary goal of this project was to examine whether HFs can be used to accurately measure change in tobacco status over time, with secondary goals of assessing the optimum timeframe for assessment and variation in accuracy by site.
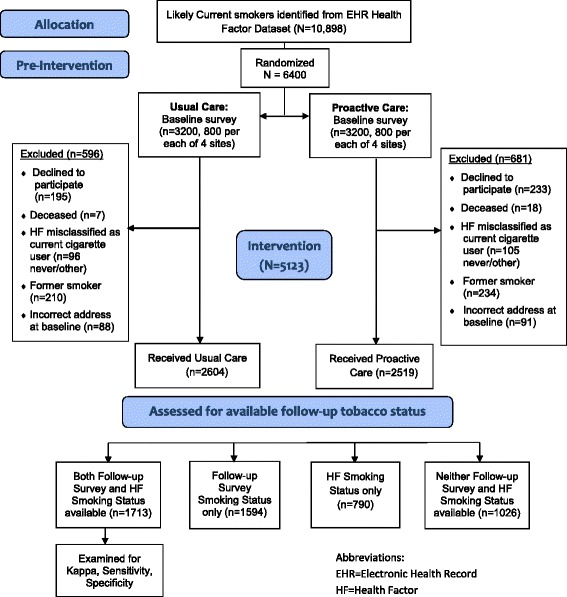
Methods: Secondary analysis of the Veterans VICTORY study, a pragmatic smoking cessation randomized controlled trial conducted from 2009 to 2011. Eligible subjects were identified via the EHR using a past 90-day HF indicating current tobacco use (for example: "CURRENT SMOKER", "CURRENTLY USES TOBACCO"). Participants were surveyed at 1 year to determine prolonged smoking abstinence. We identified HFs for tobacco status within +/- 120 days of the follow-up survey mailing date and recorded the temporally closest HF. Among subjects with both measures, we compared the two for agreement using kappa statistics and concordance.
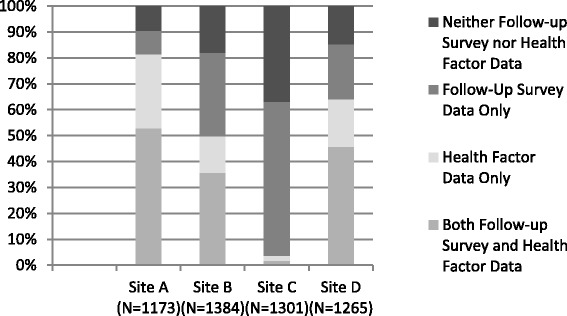
Results: 1713 subjects (33%) had both follow-up survey and HF data, 1594 (31%) had only a survey response, 790 (15%) had only HF and 1026 (20%) had neither. For subjects with both measures, there was 90% concordance and moderate agreement (Kappa 0.48, 95%CI 0.41-0.55, Sensitivity 54.4, 95%CI 41.1-67.7, Specificity 94.3, 95%CI 87.5-100.0).
Conclusions: We found high concordance but only moderate agreement by kappa statistics between HFs and survey data. The difference is likely accounted for by the natural history of quit attempts, in which patients cycle in and out of quit attempts. HFs appear to provide an accurate measure of population level quit behavior utilizing data collected in the course of clinical care.
Trial registration: ClinicalTrials.gov NCT00608426.
Keywords: Behavior change; Electronic health record; Health services; Methods; Smoking; Tobacco cessation.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the following institutional review boards: the Minneapolis VA Medical Center Institutional Review Board, the James A. Haley Veterans Hospital Institutional Review Board, the VA New York Healthcare System Institutional Review Board, and the VA Medical Center G.V. (Sonny) Montgomery Institutional Review Board. Written informed consent was obtained from participants at the time of enrollment.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- CENTERS FOR DISEASE CONTROL AND PREVENTION . The health consequences of smoking–50 years of progress: a report of the surgeon general. Rockville: US DEPARTMENT OF HEALTH AND HUMAN SERVICES; 2014. p. 171.
-
- Fiore MC, Jaen C, Baker TB, Baily WC, Benowitz NL, Curry SJ, et al. Treating tobacco use and dependence: 2008 update. Rockville: U.S. Department of Health and Human Services. Public Health Service; 2008.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
