

Prevalence of asthma among the adult general population of five Middle Eastern countries: results of the SNAPSHOT program
- PMID: 29751756
- PMCID: PMC5948696
- DOI: 10.1186/s12890-018-0621-9
Prevalence of asthma among the adult general population of five Middle Eastern countries: results of the SNAPSHOT program
Abstract
Background: Asthma is a common chronic respiratory disease leading to morbidity, mortality and impaired quality of life worldwide. Information on asthma prevalence in the Middle East is fragmented and relatively out-dated. The SNAPSHOT program was conducted to obtain updated information.
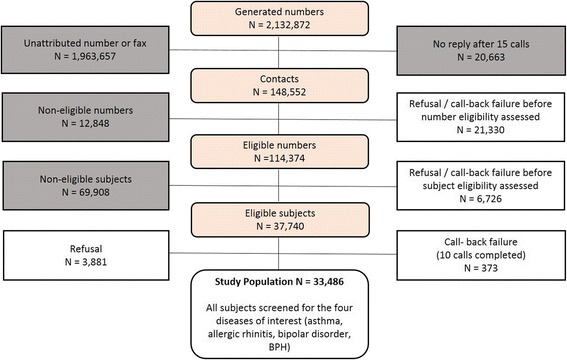
Methods: SNAPSHOT is a cross-sectional epidemiological program carried out in five Middle Eastern countries (Egypt, Turkey, Kuwait, Saudi Arabia, and the United Arab Emirates, the latter three grouped into a Gulf cluster) to collect data on asthma, allergic rhinitis, benign prostatic hyperplasia and bipolar disorder. The survey was carried out by telephone in a random sample of the adult general population with quotas defined according to country demographics. The analysis presented in this paper focuses on asthma. Subjects were screened for asthma based on criteria from the global Asthma Insights and Reality studies. Current prevalence (last 12 months) was estimated. Multivariate logistic regression analyses were used to investigate risk factors related to asthma and the association with allergic rhinitis and other co-morbidities. Quality of life was assessed using the three-level EQ-5D questionnaire.
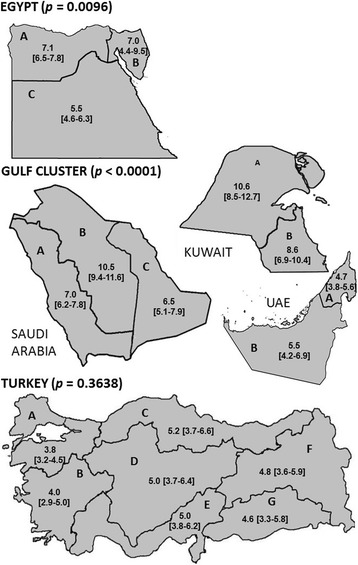
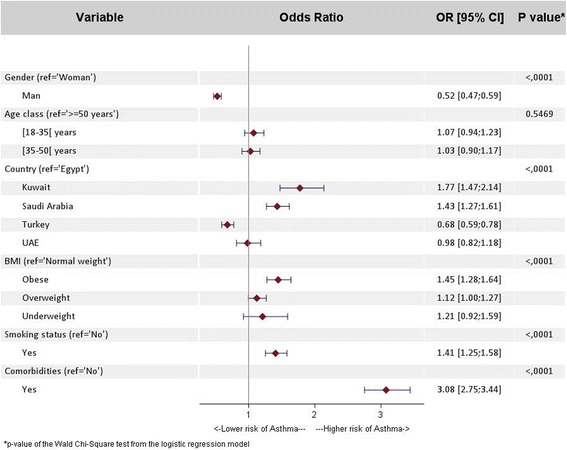
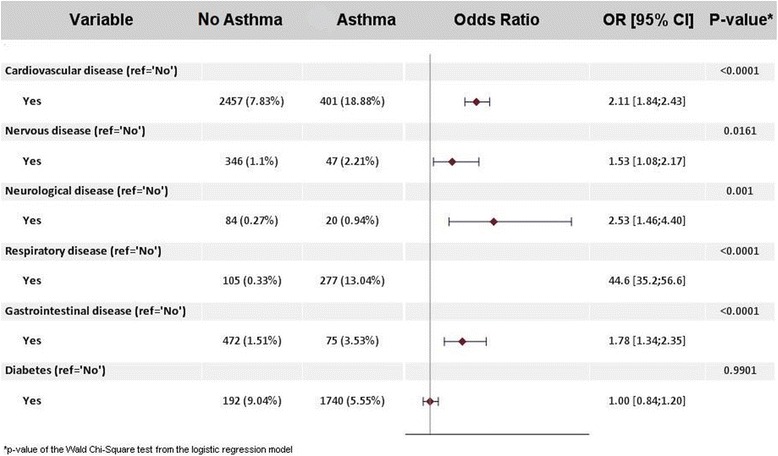
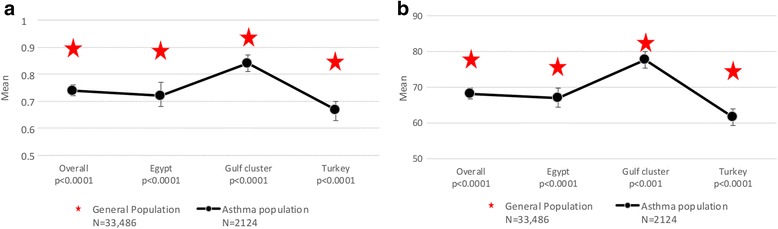
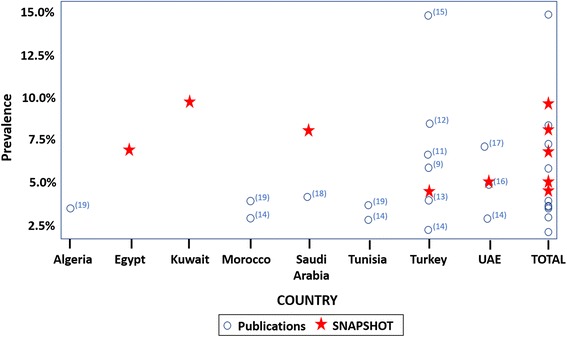
Results: 2124 out of the 33,486 subjects enrolled in the SNAPSHOT program fulfilled the criteria for asthma. The adjusted prevalence of asthma ranged from 4.4% [95% CI: 4.0-4.8%] in Turkey, to 6.7% [95% CI: 6.2-7.2%] in Egypt and 7.6% [95% CI: 7.1-8.0%] in the Gulf cluster. Prevalence was higher (p < 0.0001) in women than men and increased with age (p < 0.0001). Co-morbidities occurred more frequently in asthma subjects compared to the non-asthma population (38% vs. 15% p < 0.0001). Subjects with asthma reported a lower (p < 0.0001) EQ-VAS score (68.2 ± 22.9) compared to the general population (78.1 ± 17.5). The risk factors associated with asthma were age, gender, country, and certain co-morbidities, namely respiratory, cardiovascular, gastrointestinal, nervous, and neurological diseases.
Conclusion: The observed adjusted prevalence of asthma in the Middle East ranges from 4.4% to 7.6%, which is comparatively lower than the reported prevalence in Europe and North America. Asthma has a negative impact on quality of life, and is associated with high levels of co-morbid diseases, indicating a need for physicians to check for co-morbidities and ensure they are managed correctly in all asthma patients.
Keywords: Asthma; Co-morbidity; Middle East; Prevalence; Quality of life; SNAPSHOT.
Conflict of interest statement
Ethics approval and consent to participate
The study followed guidelines for good epidemiological practice (GEP) and pertinent local rules and regulations for each participating country. The protocol and amendments were submitted to the appropriate independent ethics committee in each country for approval. The following ethics committees approved the SNAPSHOT program: In Egypt, the Ministry of Health and Population, Central Directorate for Research and Health Development; In Kuwait, the Kuwait University Health Sciences Centre Ethical Committee; in Turkey, the Ankara University Medical Faculty Ethics Committee; and in the UAE, the Ethics and Research Committee of the University of Sharjah. In Saudi Arabia, no ethics approval was required, since SNAPSHOT was an epidemiological, cross sectional, population based study and as such is out of scope of the Saudi Food and Drug Authority (SFDA) approval and/or notification. The protocol specified that oral consent to participate in the study was required. At the start of the telephone call, subjects were asked to provide their consent to participate verbally, and this information was recorded in the CAPI system by the interviewee. Participants taking part in the study did not receive any financial compensation and participation in the study did not influence the medical management of the patient. It was not possible to link the telephone number dialled and the respondent’s data in the study database. All data collected was kept confidential and anonymous.
Competing interests
AEH, FA, and LT are employees of and shareholders in GSK, which funded the SNAPSHOT study. HT is currently also employed by GSK but at the time the study was conducted he participated in his capacity as Professor of medicine and allergy at the University of Cairo. AL is a director of MS Health, the clinical and epidemiological research company that implemented this study on behalf of GSK. AD is a director of Foxymed, a medical communication and consultancy company which participated in the design of the study and the interpretation of the results on behalf of GSK. The authors declare to have no further conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- The Global Asthma Report 2014. In.: Global asthma network; 2014.
-
- Global surveillance, prevention and control of chronic respiratory diseases: a comprehensive approach. In.: World Health Organisation; 2007.
-
- Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. The international study of asthma and allergies in childhood (ISAAC) steering committee. Lancet (London, England). 1998;351(9111):1225–32. - PubMed
-
- Variations in the prevalence of respiratory symptoms, self-reported asthma attacks, and use of asthma medication in the European Community respiratory health survey (ECRHS). Eur Respir J. 1996;9(4):687–95. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
