

Sex-specific relevance of diabetes to occlusive vascular and other mortality: a collaborative meta-analysis of individual data from 980 793 adults from 68 prospective studies
- PMID: 29752194
- PMCID: PMC6008496
- DOI: 10.1016/S2213-8587(18)30079-2
Sex-specific relevance of diabetes to occlusive vascular and other mortality: a collaborative meta-analysis of individual data from 980 793 adults from 68 prospective studies
Abstract
Background: Several studies have shown that diabetes confers a higher relative risk of vascular mortality among women than among men, but whether this increased relative risk in women exists across age groups and within defined levels of other risk factors is uncertain. We aimed to determine whether differences in established risk factors, such as blood pressure, BMI, smoking, and cholesterol, explain the higher relative risks of vascular mortality among women than among men.
Methods: In our meta-analysis, we obtained individual participant-level data from studies included in the Prospective Studies Collaboration and the Asia Pacific Cohort Studies Collaboration that had obtained baseline information on age, sex, diabetes, total cholesterol, blood pressure, tobacco use, height, and weight. Data on causes of death were obtained from medical death certificates. We used Cox regression models to assess the relevance of diabetes (any type) to occlusive vascular mortality (ischaemic heart disease, ischaemic stroke, or other atherosclerotic deaths) by age, sex, and other major vascular risk factors, and to assess whether the associations of blood pressure, total cholesterol, and body-mass index (BMI) to occlusive vascular mortality are modified by diabetes.
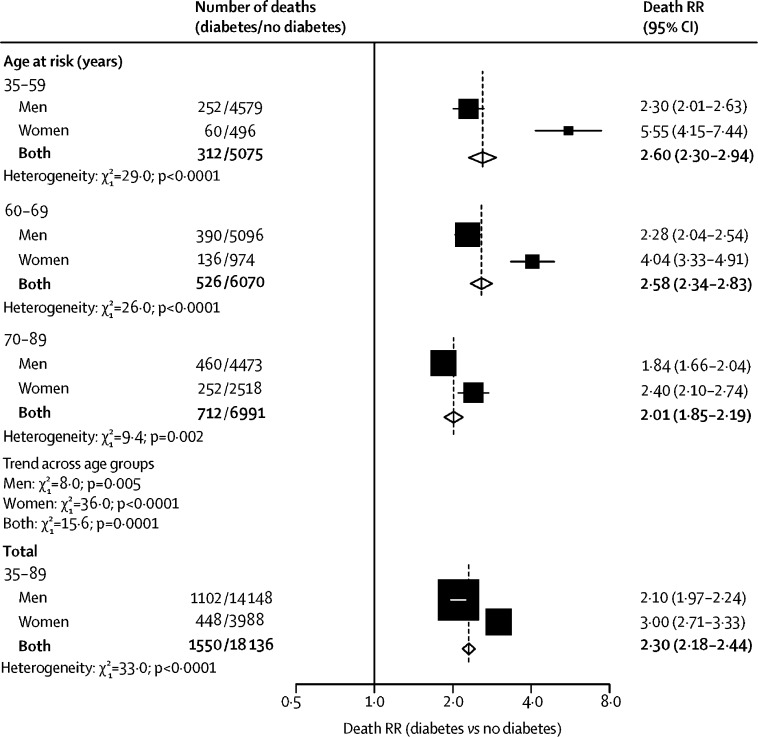
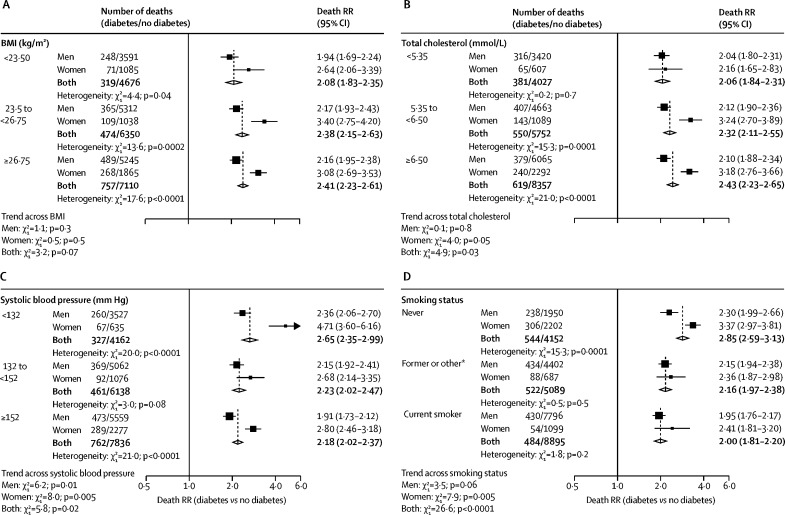
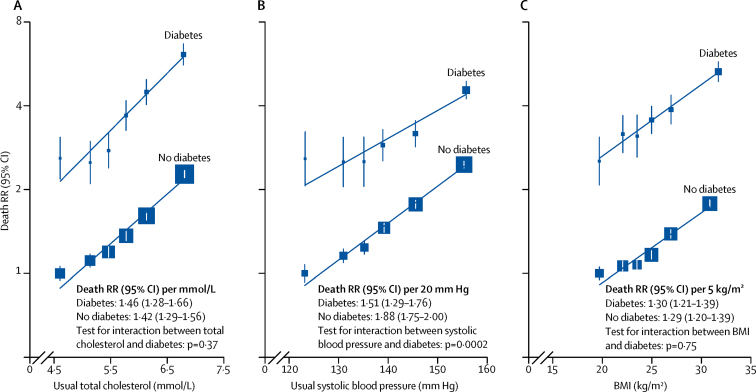
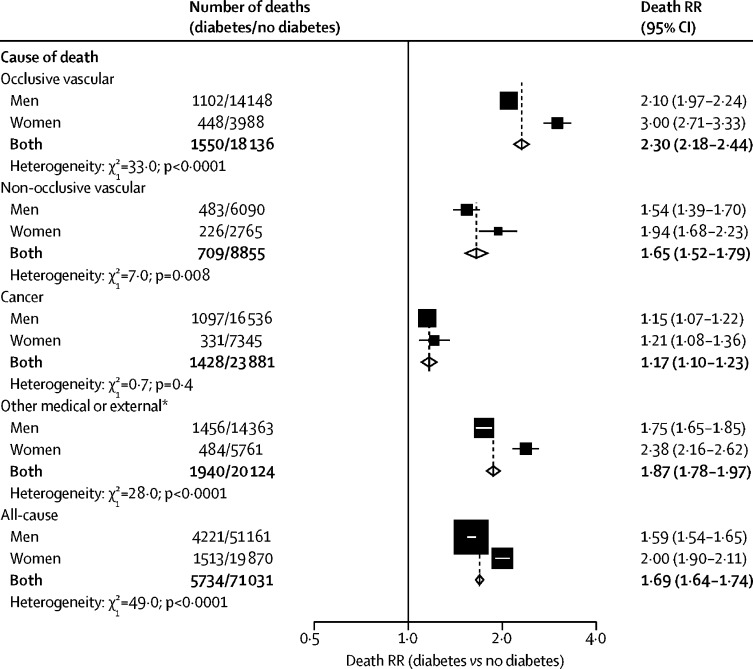
Results: Individual participant-level data were analysed from 980 793 adults. During 9·8 million person-years of follow-up, among participants aged between 35 and 89 years, 19 686 (25·6%) of 76 965 deaths were attributed to occlusive vascular disease. After controlling for major vascular risk factors, diabetes roughly doubled occlusive vascular mortality risk among men (death rate ratio [RR] 2·10, 95% CI 1·97-2·24) and tripled risk among women (3·00, 2·71-3·33; χ2 test for heterogeneity p<0·0001). For both sexes combined, the occlusive vascular death RRs were higher in younger individuals (aged 35-59 years: 2·60, 2·30-2·94) than in older individuals (aged 70-89 years: 2·01, 1·85-2·19; p=0·0001 for trend across age groups), and, across age groups, the death RRs were higher among women than among men. Therefore, women aged 35-59 years had the highest death RR across all age and sex groups (5·55, 4·15-7·44). However, since underlying confounder-adjusted occlusive vascular mortality rates at any age were higher in men than in women, the adjusted absolute excess occlusive vascular mortality associated with diabetes was similar for men and women. At ages 35-59 years, the excess absolute risk was 0·05% (95% CI 0·03-0·07) per year in women compared with 0·08% (0·05-0·10) per year in men; the corresponding excess at ages 70-89 years was 1·08% (0·84-1·32) per year in women and 0·91% (0·77-1·05) per year in men. Total cholesterol, blood pressure, and BMI each showed continuous log-linear associations with occlusive vascular mortality that were similar among individuals with and without diabetes across both sexes.
Interpretation: Independent of other major vascular risk factors, diabetes substantially increased vascular risk in both men and women. Lifestyle changes to reduce smoking and obesity and use of cost-effective drugs that target major vascular risks (eg, statins and antihypertensive drugs) are important in both men and women with diabetes, but might not reduce the relative excess risk of occlusive vascular disease in women with diabetes, which remains unexplained.
Funding: UK Medical Research Council, British Heart Foundation, Cancer Research UK, European Union BIOMED programme, and National Institute on Aging (US National Institutes of Health).
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Diabetes and cardiovascular mortality: the impact of sex.Lancet Diabetes Endocrinol. 2018 Jul;6(7):517-519. doi: 10.1016/S2213-8587(18)30111-6. Epub 2018 May 8. Lancet Diabetes Endocrinol. 2018. PMID: 29752193 No abstract available.
-
Hyperglycaemia in pregnancy and the effect of diabetes on cardiovascular risk.Lancet Diabetes Endocrinol. 2018 Aug;6(8):599. doi: 10.1016/S2213-8587(18)30208-0. Lancet Diabetes Endocrinol. 2018. PMID: 30053982 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
