

Four-Year Evolution of a Thrombophylaxis Protocol in an Enhanced Recovery After Surgery (ERAS) Program: Recent Results in 485 Patients
- PMID: 29754385
- PMCID: PMC6018584
- DOI: 10.1007/s11695-018-3299-4
Four-Year Evolution of a Thrombophylaxis Protocol in an Enhanced Recovery After Surgery (ERAS) Program: Recent Results in 485 Patients
Abstract
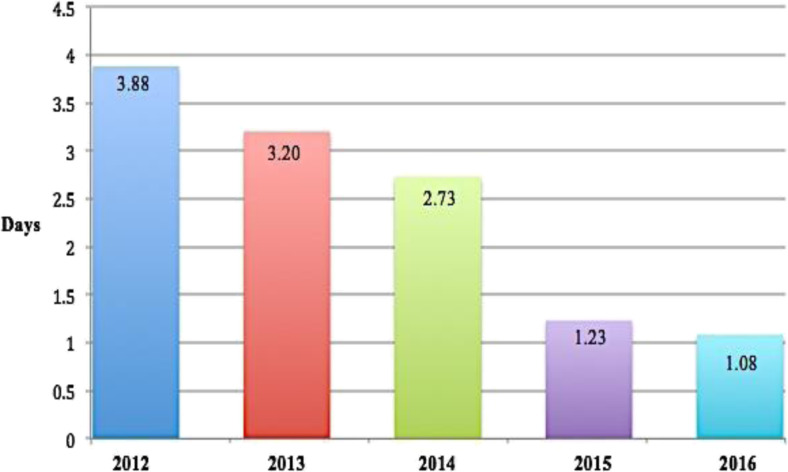
"Enhanced recovery after surgery" (ERAS) protocols may reduce morbidity, length of hospital stay (LOS), and costs. During the 4-year evolution of a bariatric ERAS protocol, we found that administration of thrombophylaxis selectively to high-risk morbidly obese patients (assessed postoperatively by Caprini score ≥ 3) undergoing omega loop gastric bypass ("mini" gastric bypass) or sleeve gastrectomy resulted in safe outcomes. Both procedures proved equally effective with this protocol. The vast majority of rapidly mobilized, low-risk patients did not appear to require antithrombotic heparin. Similar to other reported ERAS outcomes, our recent year's results in 485 patients included a mean LOS of 1.08 ± 0.64 days (range 1-14), with 460 (95.0%) discharged on day 1 and 99.6% by day 2. There were 13 30-day complications (2.7%), two reinterventions (0.4%), and no hemorrhages.
Keywords: Bariatric; ERAS; Enhanced recovery after surgery; LSG; MGB; Omega loop; Sleeve gastrectomy.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Singh P, Panwar R, Borle B, Goudra B, Trikha A, van Wagensveld B, Sinha A. Efficiency and safety effects of applying ERAS protocols to bariatric surgery: a systematic review with meta-analysis and trial sequential analysis of evidence. Obes Surg. 2017;27:489–501. doi: 10.1007/s11695-016-2442-3. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
