

Prevalent digoxin use and subsequent risk of death or hospitalization in ambulatory heart failure patients with a reduced ejection fraction-Findings from the Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training (HF-ACTION) randomized controlled trial
- PMID: 29754673
- PMCID: PMC7050977
- DOI: 10.1016/j.ahj.2018.02.004
Prevalent digoxin use and subsequent risk of death or hospitalization in ambulatory heart failure patients with a reduced ejection fraction-Findings from the Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training (HF-ACTION) randomized controlled trial
Abstract
Background: Despite more than 200 years of clinical experience and a pivotal trial, recently published research has called into question the safety and efficacy of digoxin therapy in heart failure (HF).
Methods: HF-ACTION (ClinicalTrials.gov Number: NCT00047437) enrolled 2331 outpatients with HF and an EF ≤35% between April 2003 and February 2007 and randomized them to aerobic exercise training versus usual care. Patients were grouped according to prevalent digoxin status at baseline. The association between digoxin therapy and outcomes was assessed using Cox proportional hazard and inverse-probability weighted (IPW) regression models adjusted for demographics, medical history, medications, laboratory values, quality of life, and exercise parameters.
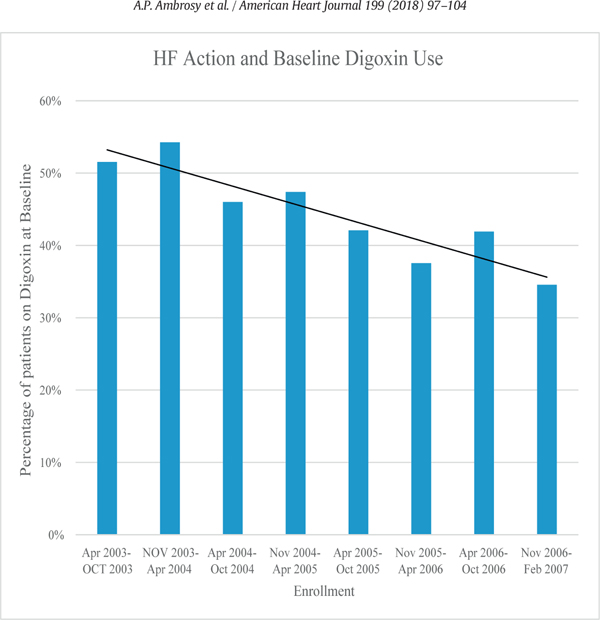
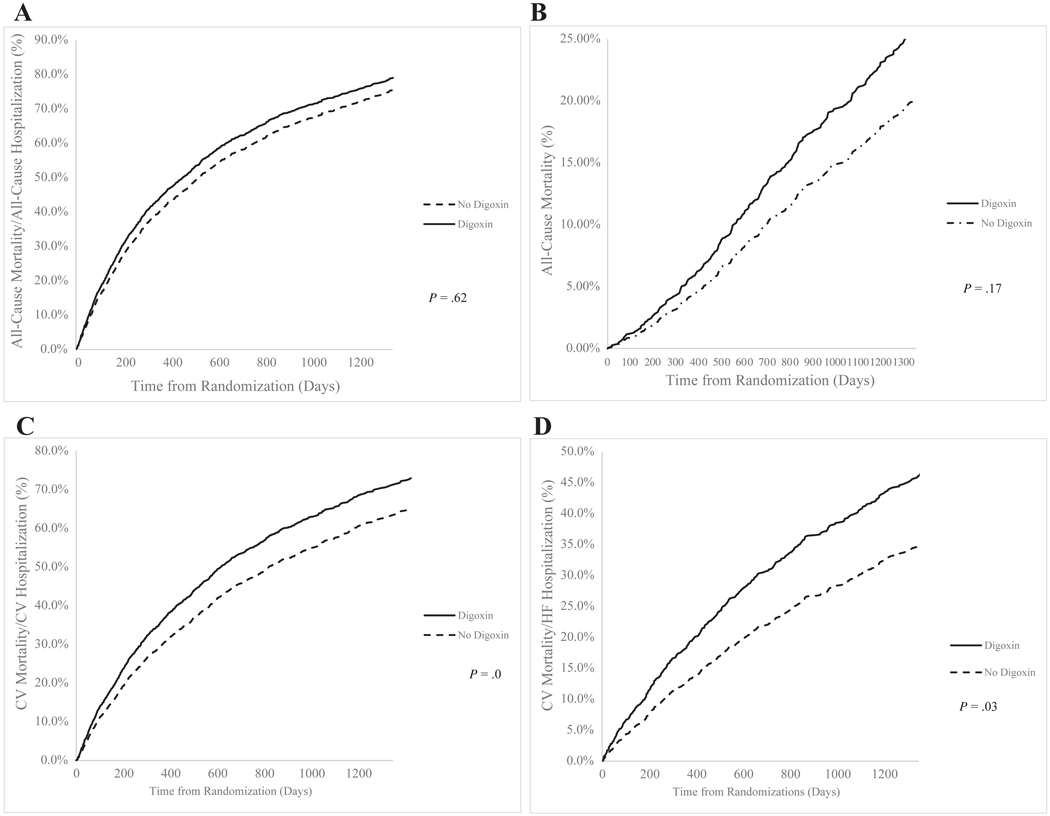
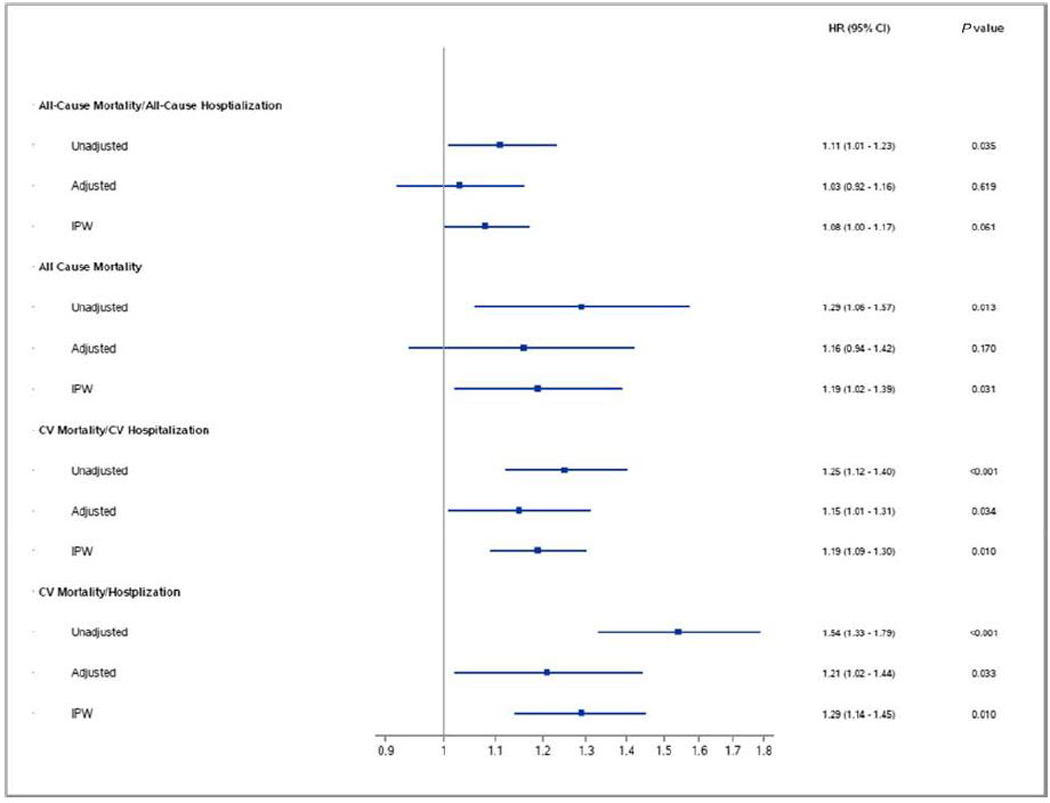
Results: The prevalence of digoxin therapy decreased from 52% during the first 6 months of enrollment to 35% at the end of the HF-ACTION trial (P <0.0001). Study participants were 59± 13 years of age, 72% were male, and approximately half had an ischemic etiology of HF. Patients receiving digoxin at baseline tended to be younger and were more likely to report New York Heart Association functional class III/IV symptoms (rather than class II) compared to those not receiving digoxin. Patients taking digoxin had worse baseline exercise capacity as measured by peak VO2 and 6-min walk test and greater impairments in health status as reflected by the Kansas City Cardiomyopathy Questionnaire. The association between digoxin and the risk of death or hospitalization differed depending on whether Cox proportional hazard (Hazard Ratio 1.03, 95% Confidence Interval 0.92-1.16; P = .62) or IPW regression models (HR 1.08, 95% CI 1.00-1.17; P = .057) were used to adjust for potential confounders.
Conclusion: Although digoxin use was associated with high-risk clinical features, the association between digoxin therapy and outcomes was dependent on the statistical methods used for multivariable adjustment. Clinical equipoise exists and additional prospective research is required to clarify the role of digoxin in contemporary clinical practice including its effects on functional capacity, quality of life, and long-term outcomes.
Copyright © 2018. Published by Elsevier Inc.
Figures
Similar articles
-
Aerobic exercise training and general health status in ambulatory heart failure patients with a reduced ejection fraction-Findings from the Heart Failure and A Controlled Trial Investigating Outcomes of Exercise Training (HF-ACTION)trial.Am Heart J. 2017 Apr;186:130-138. doi: 10.1016/j.ahj.2016.12.017. Epub 2017 Jan 19. Am Heart J. 2017. PMID: 28454828 Clinical Trial.
-
Loop diuretic adjustments in patients with chronic heart failure: Insights from HF-ACTION.Am Heart J. 2018 Nov;205:133-141. doi: 10.1016/j.ahj.2018.06.017. Epub 2018 Jul 29. Am Heart J. 2018. PMID: 30158057 Free PMC article. Clinical Trial.
-
Heart Rate or Beta-Blocker Dose? Association With Outcomes in Ambulatory Heart Failure Patients With Systolic Dysfunction: Results From the HF-ACTION Trial.JACC Heart Fail. 2016 Feb;4(2):109-115. doi: 10.1016/j.jchf.2015.09.002. Epub 2015 Oct 28. JACC Heart Fail. 2016. PMID: 26519996 Clinical Trial.
-
Digoxin and Outcomes in Patients with Heart Failure and Preserved Ejection Fraction (HFpEF) Patients: A Systematic Review and Meta- Analysis.Curr Drug Targets. 2023;24(2):191-200. doi: 10.2174/1389450123666220906093058. Curr Drug Targets. 2023. PMID: 36065922
-
Exercise-based cardiac rehabilitation in patients with reduced left ventricular ejection fraction: The Cardiac Rehabilitation Outcome Study in Heart Failure (CROS-HF): A systematic review and meta-analysis.Eur J Prev Cardiol. 2020 Jun;27(9):929-952. doi: 10.1177/2047487319854140. Epub 2019 Jun 8. Eur J Prev Cardiol. 2020. PMID: 31177833 Free PMC article.
Cited by
-
Safety profile of intravenous digoxin in Chinese patients with acute heart failure with reduced ejection fraction: a small-scale prospective cohort study.Front Pharmacol. 2023 Nov 13;14:1291896. doi: 10.3389/fphar.2023.1291896. eCollection 2023. Front Pharmacol. 2023. PMID: 38026938 Free PMC article.
-
Effects of Digoxin in Heart Failure (HF) With Reduced Ejection Fraction (EF).Cureus. 2022 Mar 2;14(3):e22778. doi: 10.7759/cureus.22778. eCollection 2022 Mar. Cureus. 2022. PMID: 35371861 Free PMC article. Review.
-
Characteristics and Outcomes of Suspected Digoxin Toxicity and Immune Fab Treatment Over the Past Two Decades-2000-2020.Am J Cardiol. 2022 Nov 15;183:129-136. doi: 10.1016/j.amjcard.2022.08.004. Epub 2022 Sep 9. Am J Cardiol. 2022. PMID: 36089419 Free PMC article.
References
-
- Ambrosy AP, Butler J, Ahmed A, et al. The use of digoxin in patients with worsening chronic heart failure: reconsidering an old drug to reduce hospital admissions. J Am Coll Cardiol 2014;63(18):1823–32. - PubMed
-
- Ambrosy AP, Gheorghiade M. Targeting digoxin dosing to serum concentration: is the bullseye too small? Eur J Heart Fail 2016;18(8):1082–4. - PubMed
-
- Ambrosy AP, Pang PS, Gheorghiade M. Digoxin for Worsening Chronic Heart Failure: Underutilized and Underrated. JACC Heart Fail 2016;4(5):365–7. - PubMed
-
- Adams KF Jr, Fonarow GC, Emerman CL, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and pre-liminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J 2005;149(2):209–16. - PubMed
-
- Gheorghiade M, Abraham WT, Albert NM, et al. Systolic blood pressure at admission, clinical characteristics, and outcomes in patients hospitalized with acute heart failure. JAMA 2006;296(18):2217–26. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
