

Decision analysis defining optimal management of clinical stage 1 high-risk nonseminomatous germ cell testicular cancer with lymphovascular invasion
- PMID: 29754945
- PMCID: PMC10182405
- DOI: 10.1016/j.urolonc.2018.03.021
Decision analysis defining optimal management of clinical stage 1 high-risk nonseminomatous germ cell testicular cancer with lymphovascular invasion
Abstract
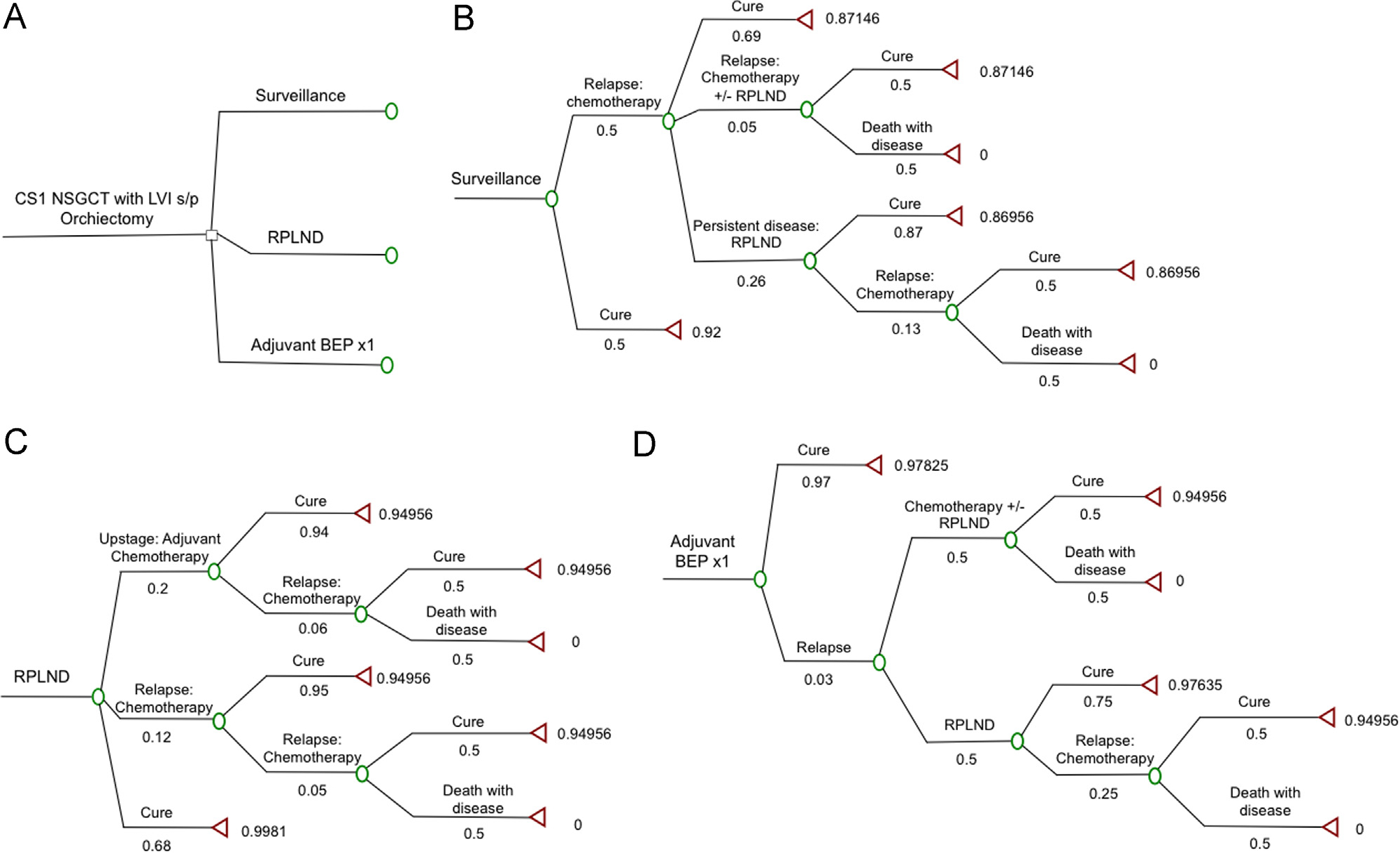
Background: Risk of recurrent disease for men with clinical stage 1 high-risk nonseminomatous germ cell testicular cancer (CS1 NSGCT) with lymphovascular invasion (LVI) after orchiectomy is 50% and current treatment options (surveillance [S], retroperitoneal lymph node dissection [RPLND], or 1 cycle of BEP [BEP ×1]) are associated with a 99% disease specific survival, therefore practice patterns vary. We performed a decision analysis using updated data of long-term complications for men with CS1 NSGCT with LVI to quantify and assess relative treatment values.
Methods: Decision analysis included previously defined utilities (via standard gamble) for posttreatment states of living from 0 (death from disease) to 1 (alive in perfect health) and updated morbidity probabilities. We quantified the values of S, RPLND, and BEP ×1 via the rollback method. Sensitivity analyses including a range of orchiectomy cure rates and utility values were performed.
Results: Estimated probabilities favoring treatment with RPLND (0.97) or BEP ×1 (0.97) were equivalent and superior to surveillance (0.88). Sensitivity analysis of orchiectomy cure rates (50%-100%) failed to find a cure rate that favored S over BEP ×1 or RPLND. Varying utility values for cure after S from 0.92 (previously defined utility) to 1 (perfect health), failed to find a viable utility state favoring S over BEP ×1 or RPLND. An orchiectomy cure rate of ≥82% would be required for S to equal treatment of either type.
Conclusions: We demonstrate that for surveillance to be superior to treatment with BEP ×1 or RPLND, the orchiectomy cure rate must be at least 82%, which is not expected in a patient population with high-risk CS1 NSGCT.
Keywords: Decision analysis; High-risk CS1 NSGCTs; Patient utilities; Treatment algorithm; Treatment value.
Copyright © 2018 Elsevier Inc. All rights reserved.
Figures



References
-
- Albers P, Albrecht W, Algaba F, et al. Guidelines on testicular cancer: 2015 update. Eur Urol 2015;68:1054–68. - PubMed
-
- Motzer RJ, Jonasch E, Agarwal N, et al. Testicular cancer, Version 2.2015. J Natl Compr Canc Netw 2015;13:772–99. - PubMed
-
- Stephenson AJ, Aprikian AG, Gilligan TD, et al. Management of low-stage nonseminomatous germ cell tumors of testis: SIU/ICUD Consensus Meeting on Germ Cell Tumors (GCT), Shanghai 2009. Urology 2011;78:S444–55. - PubMed
-
- Oldenburg J, Fosså SD, Nuver J, et al. Testicular seminoma and nonseminoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up vi125–32. Ann Oncol 2013;24(Suppl. 6). - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
