

Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting And Data System)
- PMID: 29755006
- PMCID: PMC6690492
- DOI: 10.1016/j.eururo.2018.04.029
Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting And Data System)
Abstract
Context: Management of bladder cancer (BC) is primarily driven by stage, grade, and biological potential. Knowledge of each is derived using clinical, histopathological, and radiological investigations. This multimodal approach reduces the risk of error from one particular test, but may present a staging dilemma when results conflict. Multiparametric magnetic resonance imaging (mpMRI) may improve patient care through imaging of the bladder with better resolution of the tissue planes than computed tomography and without radiation exposure.
Objective: To define a standardized approach to imaging and reporting mpMRI for BC, by developing a VI-RADS score.
Evidence acquisition: We created VI-RADS (Vesical Imaging-Reporting And Data System) through consensus using existing literature.
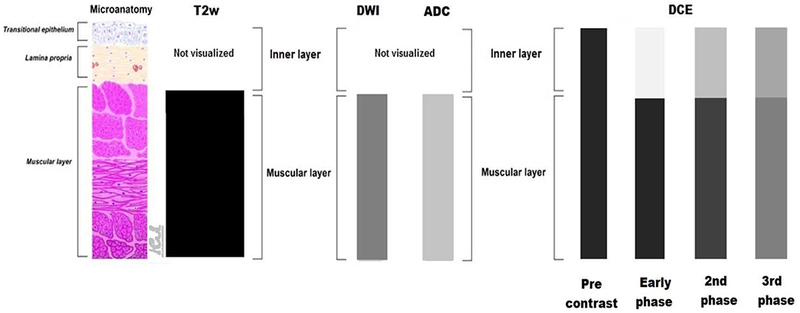
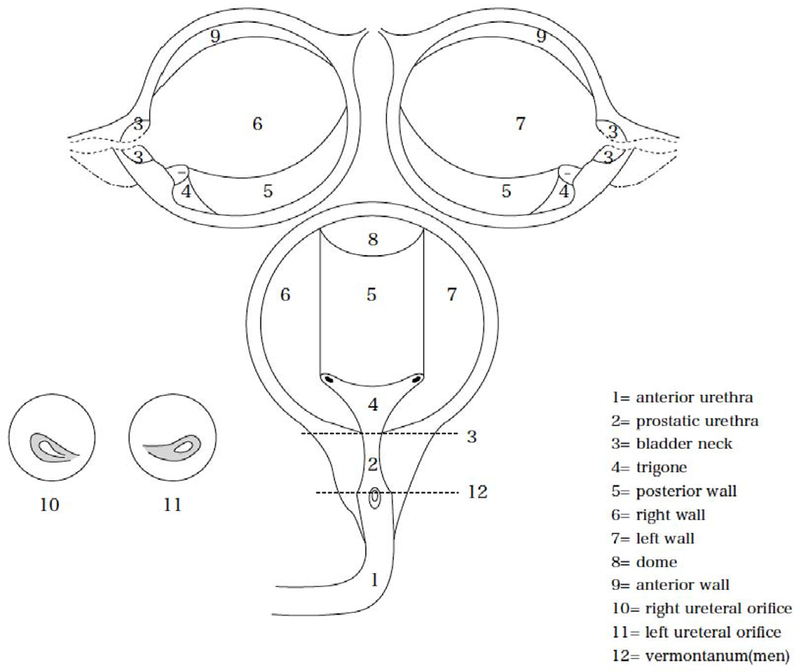
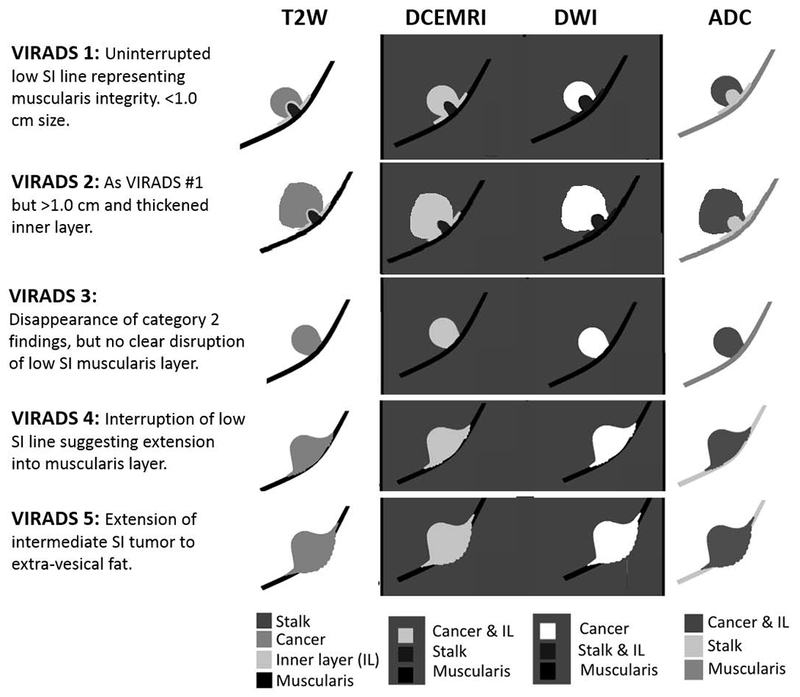
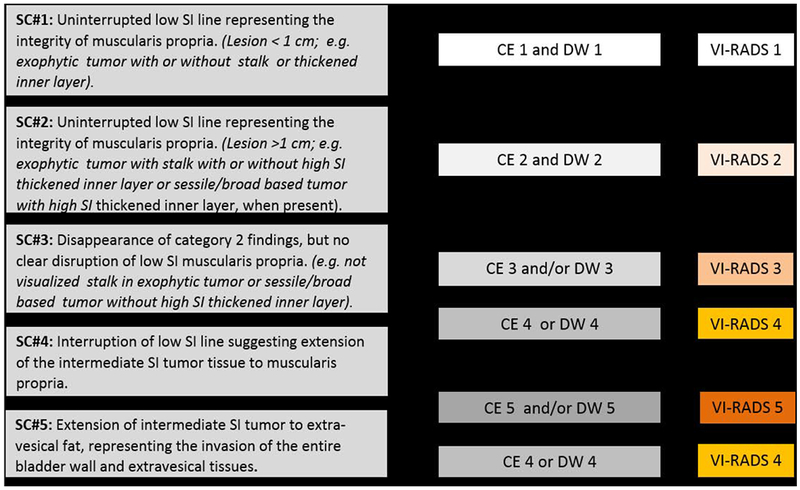
Evidence synthesis: We describe standard imaging protocols and reporting criteria (including size, location, multiplicity, and morphology) for bladder mpMRI. We propose a five-point VI-RADS score, derived using T2-weighted MRI, diffusion-weighted imaging, and dynamic contrast enhancement, which suggests the risks of muscle invasion. We include sample images used to understand VI-RADS.
Conclusions: We hope that VI-RADS will standardize reporting, facilitate comparisons between patients, and in future years, will be tested and refined if necessary. While we do not advocate mpMRI for all patients with BC, this imaging may compliment pathology or reduce radiation-based imaging. Bladder mpMRI may be most useful in patients with non-muscle-invasive cancers, in expediting radical treatment or for determining response to bladder-sparing approaches.
Patient summary: Magnetic resonance imaging (MRI) scans for bladder cancer are becoming more common and may provide accurate information that helps improve patient care. Here, we describe a standardized reporting criterion for bladder MRI. This should improve communication between doctors and allow better comparisons between patients.
Keywords: Bladder cancer; Multiparametric magnetic resonance imaging; RADS; Scoring; Staging.
Copyright © 2018 European Association of Urology. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Vesical Imaging-Reporting and Data System (VI-RADS): Added Value for Management of Bladder Cancer Patients?Eur Urol. 2018 Sep;74(3):307-308. doi: 10.1016/j.eururo.2018.06.017. Epub 2018 Jun 28. Eur Urol. 2018. PMID: 29960749 No abstract available.
-
Reply to Andrea Necchi, Antonella Messina, and Alberto Briganti's Letter to the Editor re: Valeria Panebianco, Yoshifumi Narumi, Ersan Altun, et al. Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting and Data System). Eur Urol 2018;74:294-306.Eur Urol. 2018 Nov;74(5):e109. doi: 10.1016/j.eururo.2018.06.029. Epub 2018 Jul 17. Eur Urol. 2018. PMID: 30029821 No abstract available.
-
Re: Valeria Panebianco, Yoshifumi Narumi, Ersan Altun, et al. Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting And Data System). Eur Urol 74, 2018, 294-306.Eur Urol. 2019 Feb;75(2):e27-e28. doi: 10.1016/j.eururo.2018.09.007. Epub 2018 Sep 24. Eur Urol. 2019. PMID: 30262343 No abstract available.
-
Re: Valeria Panebianco, Yoshifumi Narumi, Ersan Altun, et al. Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting And Data System). Eur Urol 2018;74:294-306: Validating VI-RADS Criteria Within Immune-oncology Strategies (VI-RADS-IO).Eur Urol. 2018 Nov;74(5):e107-e108. doi: 10.1016/j.eururo.2018.06.030. Epub 2018 Jul 4. Eur Urol. 2018. PMID: 30318068 No abstract available.
-
Reply to Jeremy Y.C. Teoh, Thomas R.W. Herrmann, and Marek Babjuk's Letter to the Editor re: Valeria Panebianco, Yoshifumi Narumi, Ersan Altun, et al. Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting and Data System). Eur Urol 2018;74:294-306.Eur Urol. 2019 Feb;75(2):e29-e30. doi: 10.1016/j.eururo.2018.09.032. Epub 2018 Nov 22. Eur Urol. 2019. PMID: 30471881 No abstract available.
References
-
- Svatek RS, Hollenbeck BK, Holmang S, et al. The economics of bladder cancer: costs and considerations of caring for this disease. Eur Urol 2014;66:253–62. - PubMed
-
- Antoni S, Ferlay J, Soerjomataram I, Znaor A, Jemal A, Bray F. Bladder cancer incidence and mortality: a global overview and recent trends. Eur Urol 2017;71:96–108. - PubMed
-
- Soukup V, Capoun O, Cohen D, et al. Prognostic performance and reproducibility of the 1973 and 2004/2016 World Health Organization grading classification systems in non-muscle-invasive bladder cancer: a European Association of Urology Non-muscle Invasive Bladder Cancer Guidelines Panel systematic review. Eur Urol 2017;72:801–13. - PubMed
-
- Linton KD, Rosario DJ, Thomas F, et al. Disease specific mortality in patients with low risk bladder cancer and the impact of cystoscopic surveillance. J Urol 2013;189:828–33. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
