

Surgical specialty and preoperative medical consultation based on commercial health insurance claims
- PMID: 29755736
- PMCID: PMC5935907
- DOI: 10.1186/s13741-018-0089-4
Surgical specialty and preoperative medical consultation based on commercial health insurance claims
Abstract
Background: Surgical patients are sometimes referred for preoperative evaluations by consultants in other medical specialties, although consultations are unnecessary for many patients, particularly for healthy patients undergoing low-risk surgeries. Surgical specialty has been shown to predict usage of preoperative consultations. However, evidence is generally limited regarding factors associated with preoperative consultations. This study evaluates surgical specialty and other predictors of preoperative consultations.
Methods: This retrospective cohort study analyzed surgery claims of 7400 privately insured patients in Washington, United States, from eight surgical specialties. We estimated log-Poisson generalized estimating equation models that regress whether a patient received a consultation on surgical specialty and covariates accounting for the data's hierarchical structure with patients nesting within surgeons, and surgeons nesting within provider organizations. Covariates include age, gender, Deyo comorbidity index, surgical risk, and geographic factors.
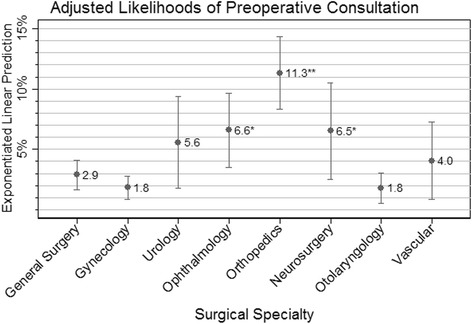
Results: Overall, 485 (6.6%) patients had a preoperative consultation. The incidence of preoperative consultation varied significantly by surgical specialty. Orthopedics, neurosurgery, and ophthalmology had 3.9 (95% CI 2.4, 6.5), 2.3 (95% CI 1.1, 4.5), and 2.3 (95% CI 1.1, 4.6) times greater adjusted likelihoods of preoperative consultation than general surgery, respectively. The adjusted likelihoods of consultation for gynecology, urology, otolaryngology, and vascular surgery were not statistically different from general surgery. The following covariates were associated with greater likelihood of preoperative consultation: greater age, higher surgical risk, having one or more comorbidities vs. none, and small rural towns vs. urban areas. More than 75% of all consultations were provided to patients with a Deyo comorbidity index of 0 or 1. Low surgical risk patients had 0.3 (95% CI 0.3, 0.5) times the likelihood of preoperative consultation of intermediate and high-risk patients overall.
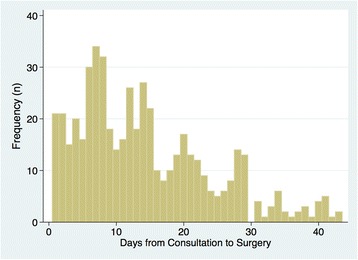
Conclusions: The likelihood of preoperative consultation varied fourfold (an absolute 9% points) across surgical specialties. Most consultations were provided to patients with low comorbidity and with low or intermediate surgical risk. To improve usage of preoperative consultations as an evidence-based practice, future research should determine how the health outcomes effects of preoperative consultations vary depending on comorbidity burden and surgical risk.
Conflict of interest statement
The University of Washington Human Subjects Division reviewed this study and determined that it is not a human subject research.We have permission from Premera Blue Cross insurance company to publish this analysis.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Patterns of preoperative consultation and surgical specialty in an integrated healthcare system.Anesthesiology. 2013 May;118(5):1028-37. doi: 10.1097/ALN.0b013e31828ea68a. Anesthesiology. 2013. PMID: 23503373 Free PMC article.
-
Preoperative consultations for medicare patients undergoing cataract surgery.JAMA Intern Med. 2014 Mar;174(3):380-8. doi: 10.1001/jamainternmed.2013.13426. JAMA Intern Med. 2014. PMID: 24366269 Free PMC article.
-
Development of an algorithm to identify preoperative medical consultations using administrative data.Med Care. 2009 Dec;47(12):1258-64. doi: 10.1097/MLR.0b013e3181bd479c. Med Care. 2009. PMID: 19890221
-
Gender diversity in UK surgical specialties: a national observational study.BMJ Open. 2022 Mar 21;12(2):e055516. doi: 10.1136/bmjopen-2021-055516. BMJ Open. 2022. PMID: 35314455 Free PMC article.
-
Virtual outreach: a randomised controlled trial and economic evaluation of joint teleconferenced medical consultations.Health Technol Assess. 2004 Dec;8(50):1-106, iii-iv. doi: 10.3310/hta8500. Health Technol Assess. 2004. PMID: 15546515 Review.
Cited by
-
Development and Validation of an Electronic Health Record-based Score for Triage to Perioperative Medicine.Ann Surg. 2023 Mar 1;277(3):e520-e527. doi: 10.1097/SLA.0000000000005284. Epub 2021 Nov 9. Ann Surg. 2023. PMID: 35129497 Free PMC article.
References
-
- Dartmouth Medical School. Center for the Evaluative Clinical Sciences . The Dartmouth atlas of health care. Chicago: American Hospital Publishing; 1996. - PubMed
-
- Devereaux PJ, Ghali WA, Gibson NE, Skjodt NM, Ford DC, Quan H, Guyatt GH. Physicians’ recommendations for patients who undergo noncardiac surgery. Clin Invest Med. 2000;23(2):116–123. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
