

Mild encephalitis/encephalopathy with a reversible splenial lesion in children
- PMID: 29757148
- PMCID: PMC5873501
- DOI: 10.5152/dir.2018.17319
Mild encephalitis/encephalopathy with a reversible splenial lesion in children
Abstract
Purpose: We aimed to present clinical and radiologic characteristics of mild encephalitis/encephalopathy with a reversible splenial lesion (MERS) in children.
Methods: Eight children (5 boys and 3 girls; median age, 5.9 years; age range, 8 months to 14.1 years) diagnosed with MERS between September 2015 and June 2017 were included in the study. We reviewed the patient's data, including demographic characteristics, prodromal and neurologic symptoms, neurologic examination, magnetic resonance imaging and electroencephalography findings, laboratory findings, treatment, and prognosis.
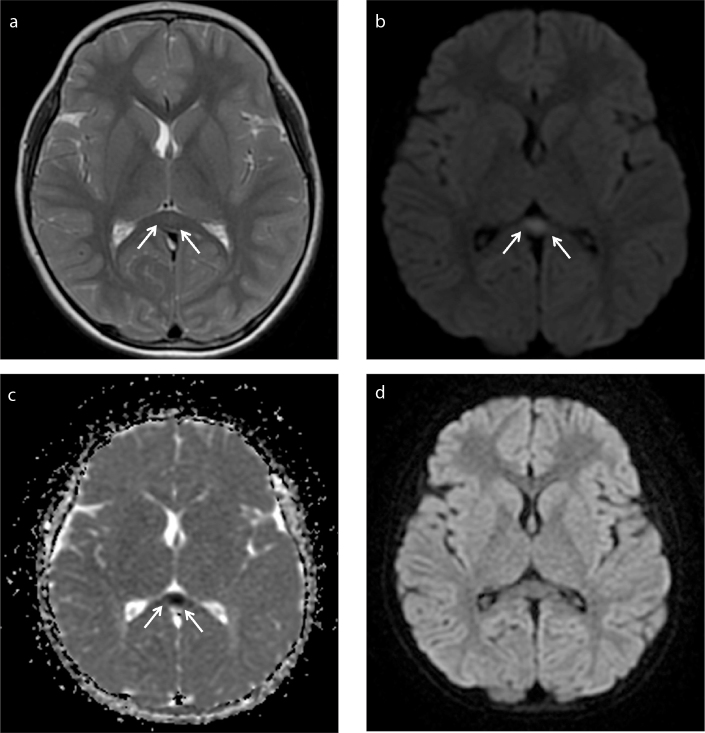
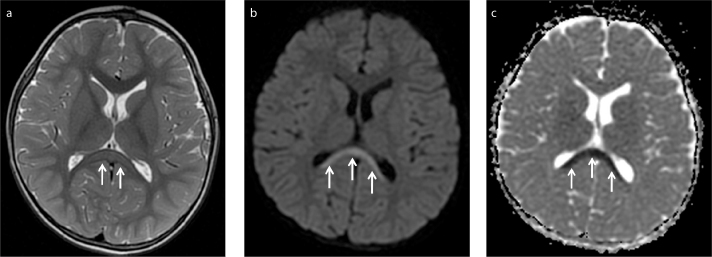
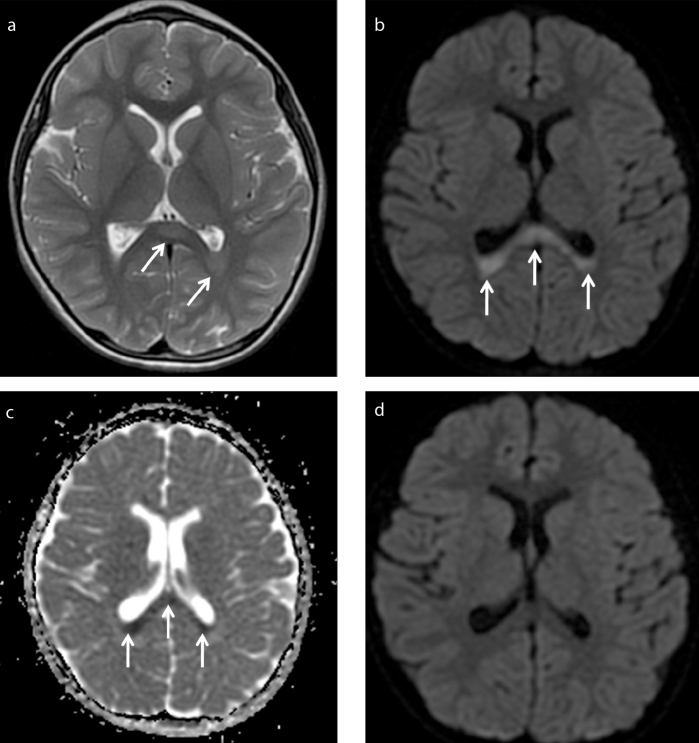
Results: Prodromal symptoms were nausea and vomiting (n=6), diarrhea (n=6), and fever (n=3). Initial neurologic symptoms were seizures (n=4), delirious behavior (n=1), drowsiness (n=1), ataxia (n=1), transient blindness (n=2), abnormal speech (n=2), and headache (n=1). Two patients had a suspected infective agent: urinary tract infection caused by Escherichia coli and gastroenteritis caused by rotavirus. Seven patients had type I lesions, comprising characteristic symmetric ovoid (n=6) and band-shaped (n=1) T2-weighted hyperintense lesions at the spenium of corpus callosum, and one patient had type II lesion with additional symmetric posterior periventricular lesions. The lesions were isointense to mildly hypointense on T1-weighted imaging and did not show enhancement. All lesions displayed restricted diffusion. In all patients, neurologic symptoms completely normalized < 48 hours from the onset of symptoms without any sequelae.
Conclusion: MERS has characteristic imaging features and favorable outcome.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures
Similar articles
-
Transient blindness associated with mild encephalitis/encephalopathy with a reversible splenial lesion (MERS): a case report and review of literature.Ital J Pediatr. 2020 Oct 12;46(1):152. doi: 10.1186/s13052-020-00918-0. Ital J Pediatr. 2020. PMID: 33046117 Free PMC article. Review.
-
Reversible splenial lesion syndrome associated with encephalitis/encephalopathy presenting with great clinical heterogeneity.BMC Neurol. 2016 Apr 18;16:49. doi: 10.1186/s12883-016-0572-9. BMC Neurol. 2016. PMID: 27089920 Free PMC article.
-
[Clinically mild encephalitis/encephalopathy with a reversible splenial lesion of corpus callosum in a child and literature review].Zhonghua Er Ke Za Zhi. 2014 Mar;52(3):218-22. Zhonghua Er Ke Za Zhi. 2014. PMID: 24824394 Review. Chinese.
-
Mild encephalitis/encephalopathy with a reversible splenial lesion: evaluation by diffusion tensor imaging. Two case reports.Neurol Med Chir (Tokyo). 2010;50(12):1118-22. doi: 10.2176/nmc.50.1118. Neurol Med Chir (Tokyo). 2010. PMID: 21206192
-
[Clinical features of mild encephalitis/encephalopathy with a reversible splenial lesion in children].Zhongguo Dang Dai Er Ke Za Zhi. 2016 Dec;18(12):1291-1295. doi: 10.7499/j.issn.1008-8830.2016.12.019. Zhongguo Dang Dai Er Ke Za Zhi. 2016. PMID: 27974125 Free PMC article. Chinese.
Cited by
-
Can plasma exchange therapy be an option for the treatment of SARS-CoV-2 Related Splenial Lesion Syndrome: Two cases from the pediatric intensive care unit.Transfus Apher Sci. 2022 Oct;61(5):103491. doi: 10.1016/j.transci.2022.103491. Epub 2022 Jun 11. Transfus Apher Sci. 2022. PMID: 35710765 Free PMC article.
-
Management of pediatric post-infectious neurological syndromes.Ital J Pediatr. 2021 Jan 25;47(1):17. doi: 10.1186/s13052-021-00968-y. Ital J Pediatr. 2021. PMID: 33494818 Free PMC article.
-
Magnetic Resonance Imaging Characteristics of Mild Encephalopathy with Reversible Splenial Lesion in A Child with Shigella Infection.Turk Arch Pediatr. 2025 May 2;60(3):349-351. doi: 10.5152/TurkArchPediatr.2025.24286. Turk Arch Pediatr. 2025. PMID: 40353779 Free PMC article. No abstract available.
-
Clinical study of recurrent mild encephalitis/encephalopathy with a reversible splenial lesion in two cases.BMC Pediatr. 2022 Jan 3;22(1):17. doi: 10.1186/s12887-021-03097-x. BMC Pediatr. 2022. PMID: 34980057 Free PMC article.
-
Transient blindness associated with mild encephalitis/encephalopathy with a reversible splenial lesion (MERS): a case report and review of literature.Ital J Pediatr. 2020 Oct 12;46(1):152. doi: 10.1186/s13052-020-00918-0. Ital J Pediatr. 2020. PMID: 33046117 Free PMC article. Review.
References
-
- Tada H, Takanashi J, Barkovich AJ, et al. Clinically mild encephalitis/encephalopathy with a reversible splenial lesion. Neurology. 2004;63:1854–1858. https://doi.org/10.1212/01.WNL.0000144274.12174.CB. - DOI - PubMed
-
- Ueda N, Minami S, Akimoto M. Mycoplasma pneumoniae-associated mild encephalitis/encephalopathy with a reversible splenial lesion: report of two pediatric cases and a comprehensive literature review. BMC Infect Dis. 2016;16:671. https://doi.org/10.1186/s12879-016-1985-1. - DOI - PMC - PubMed
-
- Fang Q, Chen L, Chen Q, Lin Z, Yang F. Clinically mild encephalitis/encephalopathy with a reversible splenial lesion of corpus callosum in Chinese children. Brain Dev. 2017;39:321–326. https://doi.org/10.1016/j.braindev.2016.10.009. - DOI - PubMed
-
- Takanashi J, Imamura A, Hayakawa F, Terada H. Differences in the time course of splenial and white matter lesions in clinically mild encephalitis/encephalopathy with a reversible splenial lesion (MERS) J Neurol Sci. 2010;292:24–27. https://doi.org/10.1016/j.jns.2010.02.013. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
