

Role of Venous Sampling in the Diagnosis of Endocrine Disorders
- PMID: 29757946
- PMCID: PMC5977153
- DOI: 10.3390/jcm7050114
Role of Venous Sampling in the Diagnosis of Endocrine Disorders
Abstract
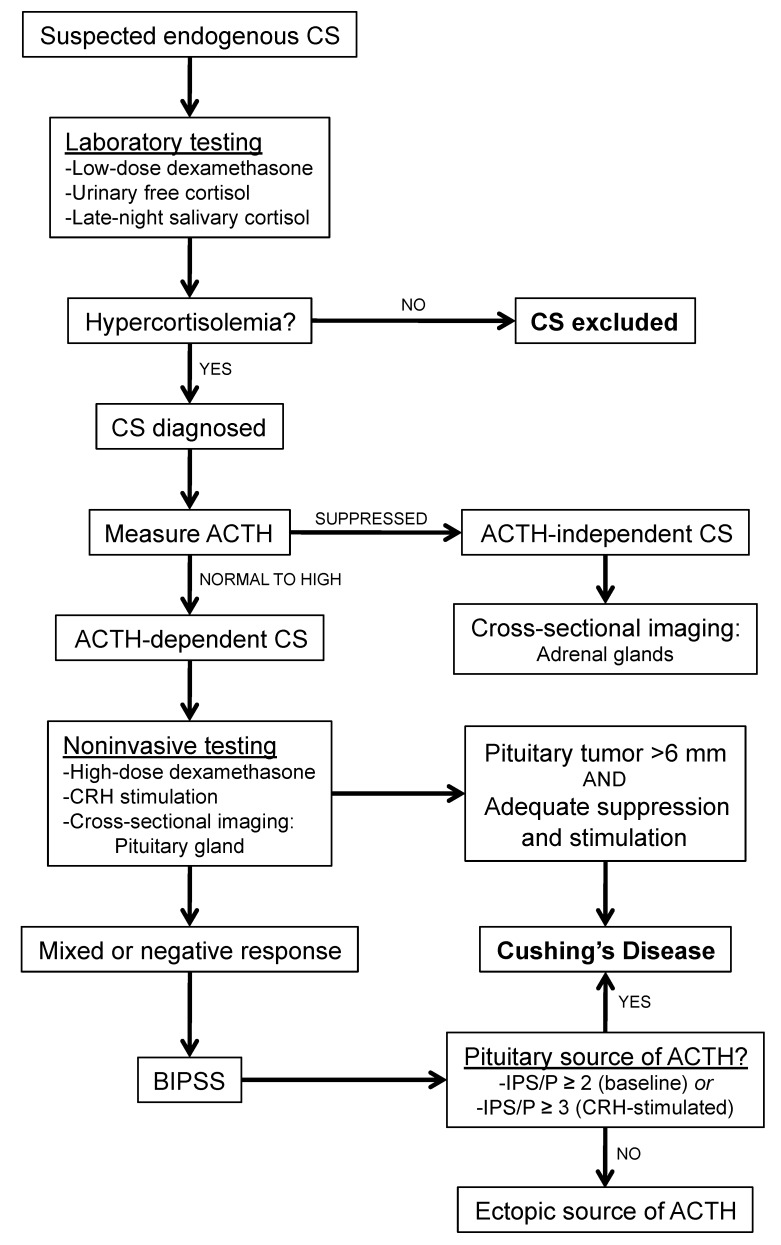
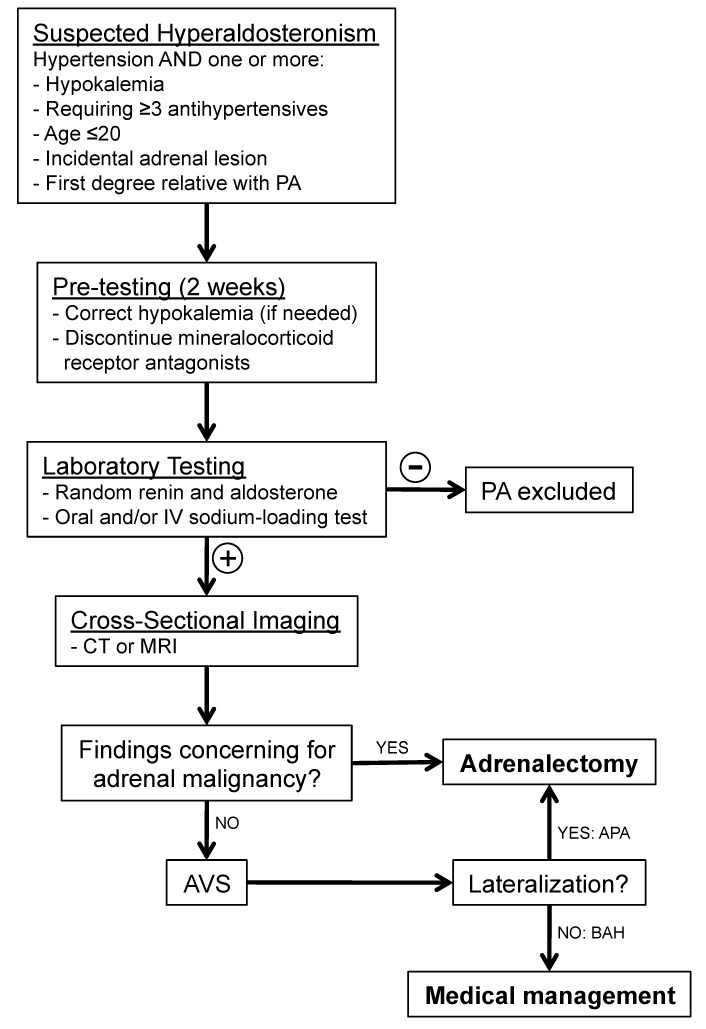
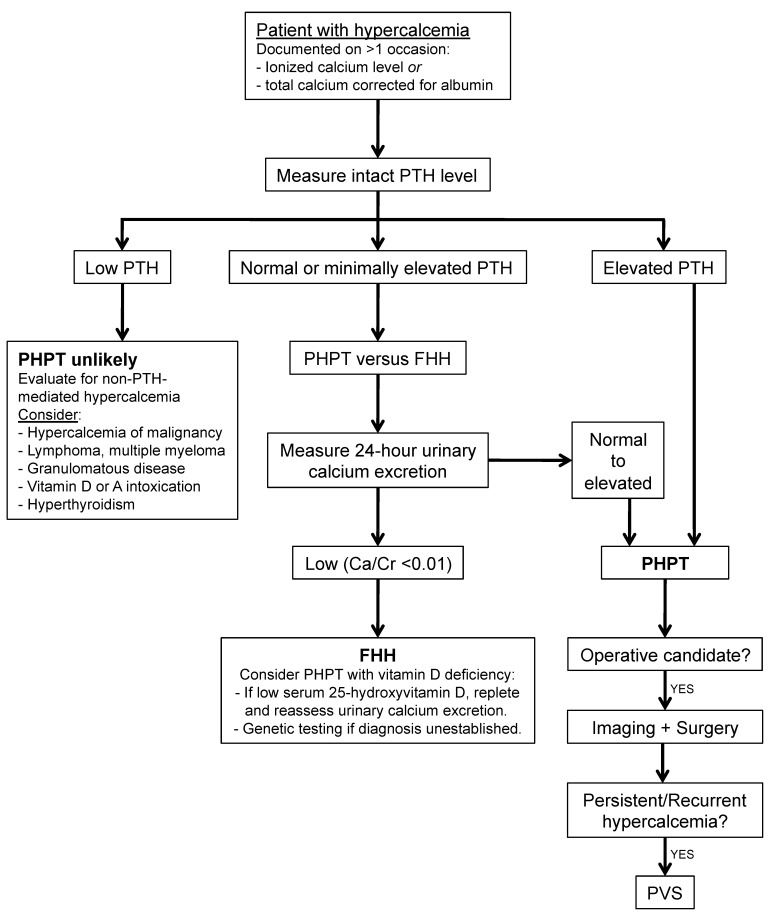
Venous sampling is the gold standard for localizing abnormal hormone secretion in several endocrine disorders. The most common indication for venous sampling is in the workup of primary aldosteronism, adrenocorticotropic hormone-dependent Cushing's syndrome, and hyperparathyroidism. In experienced hands, venous sampling is safe and accurate. This review discusses the role of venous sampling in the workup of endocrine disease, describing the underlying anatomy and pathophysiology, as an understanding of these concepts is essential for technical and clinical success.
Keywords: Cushing’s disease; adrenal vein; hyperparathyroidism; inferior petrosal sinus; primary aldosteronism; venous sampling.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




Similar articles
-
Pituitary tumour localization in patients with Cushing's disease by magnetic resonance imaging. Is there a place for petrosal sinus sampling?Clin Endocrinol (Oxf). 1994 Jan;40(1):87-92. doi: 10.1111/j.1365-2265.1994.tb02448.x. Clin Endocrinol (Oxf). 1994. PMID: 8306486
-
Jugular venous sampling: an alternative to petrosal sinus sampling for the diagnostic evaluation of adrenocorticotropic hormone-dependent Cushing's syndrome.J Clin Endocrinol Metab. 2004 Aug;89(8):3795-800. doi: 10.1210/jc.2003-032014. J Clin Endocrinol Metab. 2004. PMID: 15292307 Clinical Trial.
-
Preliminary observations using endocrine markers of pituitary venous dilution during bilateral simultaneous inferior petrosal sinus catheterization in Cushing's syndrome: is combined CRF and TRH stimulation of value?Clin Endocrinol (Oxf). 1993 Dec;39(6):681-6. doi: 10.1111/j.1365-2265.1993.tb02427.x. Clin Endocrinol (Oxf). 1993. PMID: 8287587
-
The role of inferior petrosal sinus sampling in the diagnostic localization of Cushing's disease.Neurosurg Focus. 2007;23(3):E2. doi: 10.3171/foc.2007.23.3.3. Neurosurg Focus. 2007. PMID: 17961020 Review.
-
The current role of venous sampling in the localization of endocrine disease.Cardiovasc Intervent Radiol. 2007 Jul-Aug;30(4):555-70. doi: 10.1007/s00270-007-9028-3. Cardiovasc Intervent Radiol. 2007. PMID: 17546403 Review.
Cited by
-
68Ga-pentixafor PET/CT in guiding surgical management of primary aldosteronism.J Clin Transl Endocrinol. 2025 Jan 25;39:100384. doi: 10.1016/j.jcte.2025.100384. eCollection 2025 Mar. J Clin Transl Endocrinol. 2025. PMID: 39926105 Free PMC article.
-
Determination of adrenal hypersecretion in primary Aldosteronism without aldosterone-production adenomas.BMC Endocr Disord. 2021 May 31;21(1):114. doi: 10.1186/s12902-021-00770-1. BMC Endocr Disord. 2021. PMID: 34059026 Free PMC article.
-
Atypical presentations of parathyroid gland pathology: A pictorial review.Eur J Radiol Open. 2019 Nov 8;6:320-329. doi: 10.1016/j.ejro.2019.10.001. eCollection 2019. Eur J Radiol Open. 2019. PMID: 31737749 Free PMC article.
-
Selective venous sampling for secondary hypertension.Hypertens Res. 2024 Jul;47(7):1766-1778. doi: 10.1038/s41440-024-01699-3. Epub 2024 May 15. Hypertens Res. 2024. PMID: 38750220 Review.
References
-
- Deipolyi A., Oklu R. Bilateral inferior petrosal sinus sampling in the diagnosis of Cushing disease. J. Vasc. Diagn. 2015;3:1–7.
-
- Sugg S.L., Fraker D.L., Alexander H.R., Doppman J.L., Miller D.L., Chang R., Skarulis M.C., Marx S.J., Spiegel A.M., Norton J.A. Prospective evaluation of selective venous sampling for parathyroid hormone concentration in patients undergoing reoperations for primary hyperparathyroidism. Surgery. 1993;114:1004–1010. - PubMed
-
- Kumar V., Abbas A.K., Fausto N., Aster J.C. Robbins and Cotran Pathologic Basis of Disease, Professional Edition e-Book. Elsevier Health Sciences; Philadelphia, PA, USA: 2014.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
