

Impact of Thrombotic Microangiopathy on Renal Outcomes and Survival after Hematopoietic Stem Cell Transplantation
- PMID: 29758394
- PMCID: PMC6230502
- DOI: 10.1016/j.bbmt.2018.05.010
Impact of Thrombotic Microangiopathy on Renal Outcomes and Survival after Hematopoietic Stem Cell Transplantation
Abstract
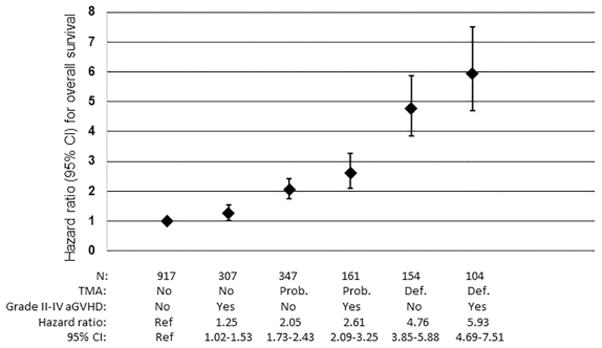
Transplantation-associated thrombotic microangiopathy (TA-TMA) is a serious complication of hematopoietic stem cell transplantation (HSCT). We characterized the incidence, risk factors, and long-term outcomes associated with TA-TMA by performing a comprehensive review of all adult patients (n = 1990) undergoing allogeneic HSCT at the Dana Farber Cancer Institute/Brigham and Women's Hospital between 2005 and 2013. Using the City of Hope criteria, we identified 258 patients (13%) with "definite" TMA and 508 patients (26%) with "probable" TMA. Mismatched donor transplantation (subdistribution hazard ratio [sHR], 1.79; 95% confidence interval [CI], 1.17 to 2.75; P = .007), sirolimus-containing graft-versus-host disease prophylaxis (sHR, 1.73; 95% CI, 1.29 to 2.34; P < .001), myeloablative conditioning (sHR, 1.93, 95% CI, 1.38 to 2.68; P < .001), and high baseline lactate dehydrogenase (LDH) level (sHR, 1.64; 95% CI, 1.26 to 2.13; P < .001) were associated with definite TMA. Moreover, positive cytomegalovirus serostatus (sHR, 1.41; 95% CI, 1.16 to 1.71; P < .001), high and very high disease risk index (sHR, 1.48; 95% CI, 1.12 to 1.96, P = .007), and high baseline LDH level (sHR, 1.25; 95% CI, 1.05 to 1.49; P = .011) were associated with probable TMA. In multivariable analyses, definite and probable TMA were each independently associated with higher mortality (HR, 5.24; 95% CI, 4.43 to 6.20 and HR, 2.12; 95% CI, 1.84 to 2.44, respectively), and long-term kidney dysfunction (HR, 5.43; 95% CI, 4.61 to 6.40 and HR, 2.20; 95% CI, 1.92 to 2.51, respectively). Definite and probable TMA were also independently associated with an increased risk of nonrelapse mortality and shorter progression-free survival. Our findings indicate that TA-TMA is common following HSCT and is independently associated with increased risk of death and kidney dysfunction.
Keywords: Allogeneic; Hematopoietic stem cell transplantation; Renal outcome; Survival; Thrombotic microangiopathies.
Copyright © 2018 The American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures





References
-
- George JN, Nester CM. Syndromes of thrombotic microangiopathy. N Engl J Med. 2014;371(7):654–666. - PubMed
-
- Noris M, Remuzzi G. Atypical hemolytic-uremic syndrome. N Engl J Med. 2009;361(17):1676–1687. - PubMed
-
- Ho VT, Cutler C, Carter S, et al. Blood and marrow transplant clinical trials network toxicity committee consensus summary: thrombotic microangiopathy after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2005;11(8):571–575. - PubMed
-
- George JN, Li X, McMinn JR, Terrell DR, Vesely SK, Selby GB. Thrombotic thrombocytopenic purpura-hemolytic uremic syndrome following allogeneic HPC transplantation: a diagnostic dilemma. Transfusion. 2004;44(2):294–304. - PubMed
-
- Oran B, Donato M, Aleman A, et al. Transplant-associated microangiopathy in patients receiving tacrolimus following allogeneic stem cell transplantation: risk factors and response to treatment. Biol Blood Marrow Transplant. 2007;13(4):469–477. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
