

Drug-eluting stents versus bare-metal stents in saphenous vein grafts: a double-blind, randomised trial
- PMID: 29759512
- PMCID: PMC6402785
- DOI: 10.1016/S0140-6736(18)30801-8
Drug-eluting stents versus bare-metal stents in saphenous vein grafts: a double-blind, randomised trial
Abstract
Background: Few studies have examined the efficacy of drug-eluting stents (DES) for reducing aortocoronary saphenous vein bypass graft (SVG) failure compared with bare-metal stents (BMS) in patients undergoing stenting of de-novo SVG lesions. We assessed the risks and benefits of the use of DES versus BMS in de-novo SVG lesions.
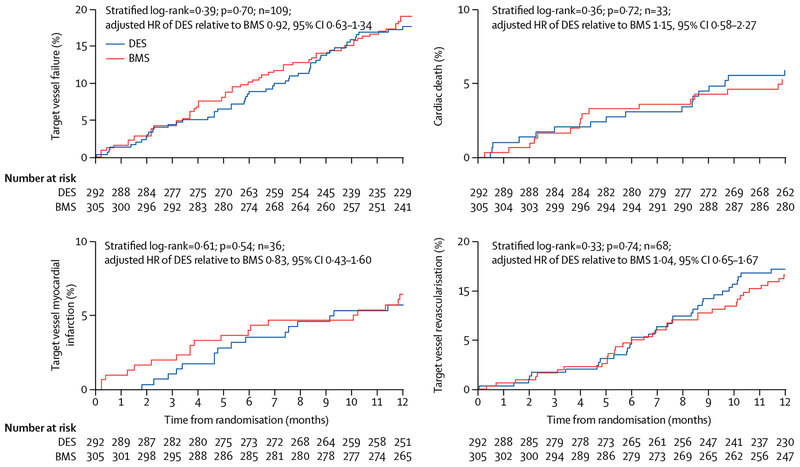
Methods: Patients were recruited to our double-blind, randomised controlled trial from 25 US Department of Veterans Affairs centres. Eligible participants were aged at least 18 years and had at least one significant de-novo SVG lesion (50-99% stenosis of a 2·25-4·5 mm diameter SVG) requiring percutaneous coronary intervention with intent to use embolic protection devices. Enrolled patients were randomly assigned, in a 1:1 ratio, by phone randomisation system to receive a DES or BMS. Randomisation was stratified by presence or absence of diabetes and number of target SVG lesions requiring percutaneous coronary intervention (one or two or more) within each participating site by use of an adaptive scheme intended to balance the two stent type groups on marginal totals for the stratification factors. Patients, referring physicians, study coordinators, and outcome assessors were masked to group allocation. The primary endpoint was the 12-month incidence of target vessel failure, defined as the composite of cardiac death, target vessel myocardial infarction, or target vessel revascularisation. The DIVA trial is registered with ClinicalTrials.gov, number NCT01121224.
Findings: Between Jan 1, 2012, and Dec 31, 2015, 599 patients were randomly assigned to the stent groups, and the data for 597 patients were used. The patients' mean age was 68·6 (SD 7·6) years, and 595 (>99%) patients were men. The two stent groups were similar for most baseline characteristics. At 12 months, the incidence of target vessel failure was 17% (51 of 292) in the DES group versus 19% (58 of 305) in the BMS group (adjusted hazard ratio 0·92, 95% CI 0·63-1·34, p=0·70). Between-group differences in the components of the primary endpoint, serious adverse events, or stent thrombosis were not significant. Enrolment was stopped before the revised target sample size of 762 patients was reached.
Interpretation: In patients undergoing stenting of de-novo SVG lesions, no significant differences in outcomes between those receiving DES and BMS during 12 months of follow-up were found. The study results have important economic implications in countries with high DES prices such as the USA, because they suggest that the lower-cost BMS can be used in SVG lesions without compromising either safety or efficacy.
Funding: US Department of Veterans Affairs Cooperative Studies Program.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests
ESB consults for and receives speaker honoraria from Abbott Vascular, Amgen, Asahi, Boston Scientific, Cardinal Health, CSI, Elsevier, GE Healthcare, Medicure, Medtronic, and Nitiloop, and receives research support from Boston Scientific, InfraRedx and Osprey. ESB’s spouse was an employee of Medtronic. DLB is an advisory board member of Cardax, Elsevier Practice Update Cardiology, Medscape Cardiology, and Regado Biosciences; is on the board of directors of Boston VA Research Institute and Society of Cardiovascular Patient Care; is chair of the American Heart Association Quality Oversight Committee; is on the data monitoring committees of Cleveland Clinic, Duke Clinical Research Institute, Harvard Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine, and Population Health Research Institute; receives honoraria from the American College of Cardiology, Belvoir Publications, Duke Clinical Research Institute, Harvard Clinical Research Institute, HMP Communications, Journal of the American College of Cardiology, Population Health Research Institute, Slack Publications, Society of Cardiovascular Patient Care, and WebMD; is deputy editor of Clinical Cardiology, and chair of the NCDR-ACTION registry steering committee and VA CART research and publications committee; receives research funding from Abbott, Amarin, Amgen, AstraZeneca, Bristol-Myers Squibb, Chiesi, Eisai, Ethicon, Forest Laboratories, Ironwood, Ischemix, Lilly, Medtronic, Pfizer, Roche, Sanofi Aventis, and The Medicines Company; receives royalties from Elsevier; is a site co-investigator for Biotronik, Boston Scientific, and St Jude Medical (now Abbott); is a trustee of the American College of Cardiology; and does unfunded research for FlowCo, Merck, PLx Pharma, and Takeda. SG receives research support from the National Institutes of Health, the VA Cooperative Studies Program, the Arizona Biomedical Research Commission, and Merck Pharmaceuticals, and is the co-founder of Avery Therapeutic. SVR consults for Medtronic. KS consults for Medeon Bio Inc, TransAortic Medical, and Terumo, and receives research support from Siemens Medical Systems and Medinol. AAB consults for the American College of Cardiology. SG receives research grants from Edwards Lifesciences and VA Office of Research and Development, and consults for Medtronic, Boston Scientific, Osprey Medical, and Surmodics. FL is a speaker for Abbott Vascular, and consults for Medicure. EA consults for Abbott Vascular, Boston Scientific, Cardiovascular Systems, Medtronic, and Spectranetics. BVR receives a research grant from InfraRedx and the Spectranetics Corporation, and salary support from the VA Cooperative Studies Program. YL consults for PTC Therapeutics and PaxVax. SB receives speaker honoraria from AstraZeneca, CSI, Gore, and Medtronic, and institutional research grants from Boston Scientific Corporation, and Merck. All other authors declare no competing interests.
Figures

Comment in
-
Stents in saphenous vein grafts.Lancet. 2018 May 19;391(10134):1967-1968. doi: 10.1016/S0140-6736(18)30937-1. Epub 2018 May 11. Lancet. 2018. PMID: 29759511 No abstract available.
-
Drug-eluting stents versus bare-metal stents for vein-graft PCI.Nat Rev Cardiol. 2018 Aug;15(8):442. doi: 10.1038/s41569-018-0042-8. Nat Rev Cardiol. 2018. PMID: 29867189 No abstract available.
-
Taking care of the soldiers.J Thorac Dis. 2018 Nov;10(Suppl 33):S4002-S4005. doi: 10.21037/jtd.2018.09.25. J Thorac Dis. 2018. PMID: 30631539 Free PMC article. No abstract available.
-
Second-generation drug-eluting stents versus bare-metal stents in saphenous vein grafts: is the choice more complicated than before?J Thorac Dis. 2019 Mar;11(Suppl 3):S385-S389. doi: 10.21037/jtd.2018.12.23. J Thorac Dis. 2019. PMID: 30997227 Free PMC article. No abstract available.
-
Drug eluting stents versus bare metal stents for the treatment of saphenous vein grafts failure: learnings from the DIVA trial.J Thorac Dis. 2019 Mar;11(Suppl 3):S399-S403. doi: 10.21037/jtd.2018.11.123. J Thorac Dis. 2019. PMID: 30997231 Free PMC article. No abstract available.
-
Drug-eluting stents versus bare-metal stents for saphenous vein graft interventions.J Thorac Dis. 2019 May;11(Suppl 9):S1257-S1260. doi: 10.21037/jtd.2019.02.50. J Thorac Dis. 2019. PMID: 31245102 Free PMC article. No abstract available.
-
Trial Sequential Analysis of Drug-Eluting Stents Versus Bare-Metal Stents in Saphenous Vein Graft Intervention.Am J Cardiol. 2019 Sep 1;124(5):823-824. doi: 10.1016/j.amjcard.2019.05.043. Epub 2019 Jun 6. Am J Cardiol. 2019. PMID: 31272706 No abstract available.
References
-
- Hall MJ, Levant S, DeFrances CJ. Trends in inpatient hospital deaths: National Hospital Discharge Survey, 2000–2010. NCHS Data Brief 2013; 2013: 1–8. - PubMed
-
- Widimsky P, Straka Z, Stros P, et al. One-year coronary bypass graft patency: a randomized comparison between off-pump and on-pump surgery angiographic results of the PRAGUE-4 trial. Circulation 2004; 110: 3418–23. - PubMed
-
- Alexander JH, Hafley G, Harrington RA, et al. Efficacy and safety of edifoligide, an E2F transcription factor decoy, for prevention of vein graft failure following coronary artery bypass graft surgery: PREVENT IV: a randomized controlled trial. JAMA 2005; 294: 2446–54. - PubMed
-
- Brilakis ES, Rao SV, Banerjee S, et al. Percutaneous coronary intervention in native arteries versus bypass grafts in prior coronary artery bypass grafting patients a report from the national cardiovascular data registry. JACC Cardiovasc Interv 2011; 4: 844–50. - PubMed
-
- Goldman S, Zadina K, Moritz T, et al. Long-term patency of saphenous vein and left internal mammary artery grafts after coronary artery bypass surgery results from a Department of Veterans Affairs cooperative study. J Am Coll Cardiol 2004; 44: 2149–56. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
