

Differences in Prehospital Patient Assessments for Pediatric Versus Adult Patients
- PMID: 29759850
- PMCID: PMC7073459
- DOI: 10.1016/j.jpeds.2018.03.069
Differences in Prehospital Patient Assessments for Pediatric Versus Adult Patients
Abstract
Objective: To evaluate whether completion of vital signs assessments in pediatric transports by emergency medical services (EMS) differs by patient age.
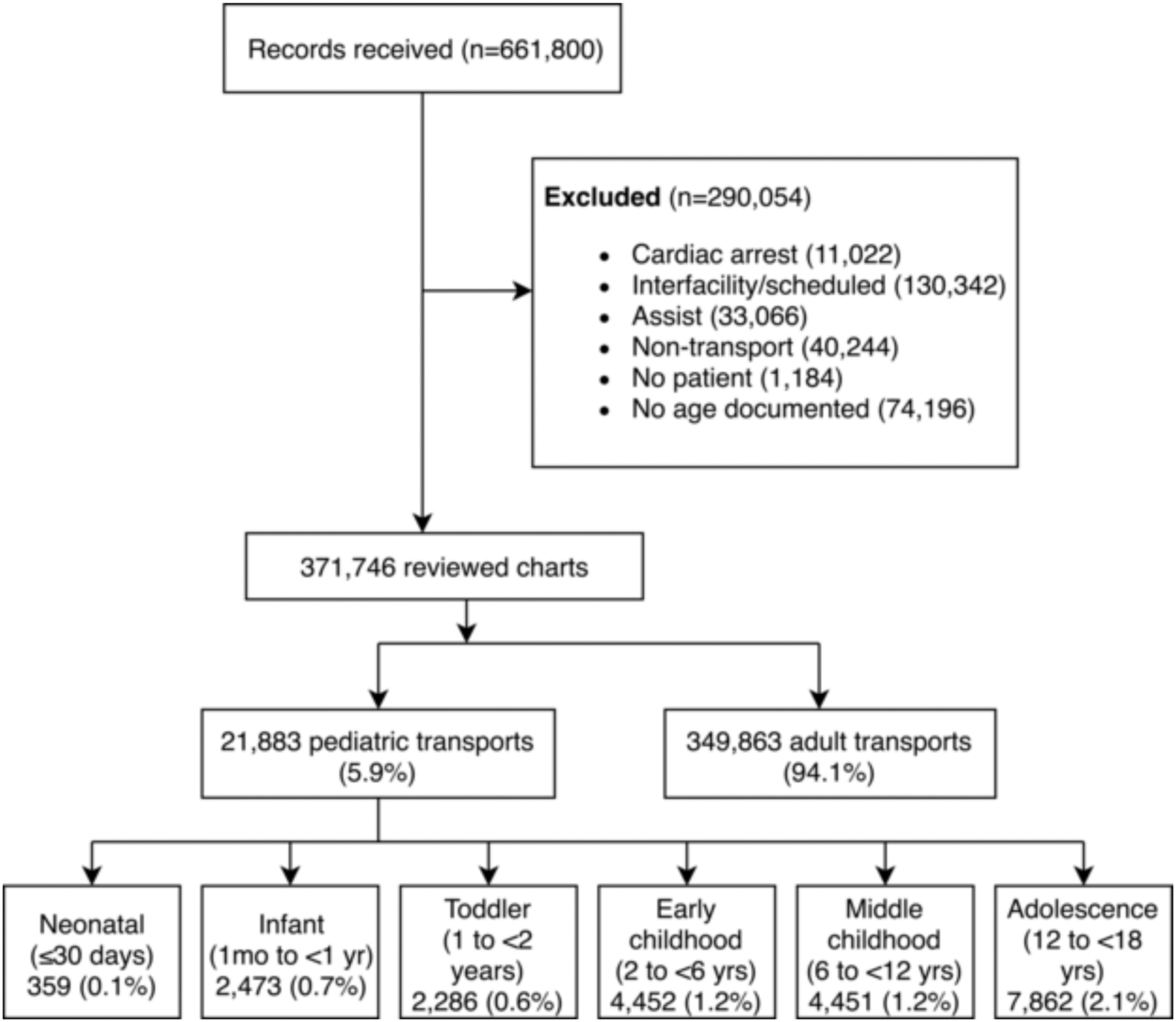
Study design: We reviewed records by 20 agencies in a regional EMS system in Southwestern Pennsylvania between April 1, 2013 and December 31, 2016. We abstracted demographics, vital signs (systolic blood pressure, heart rate, respiratory rate), clinical, and transport characteristics. We categorized age as neonates (≤30 days), infants (1 month to <1 year), toddler (1 to <2 years), early childhood (2 to <6 years), middle childhood (6 to <12 years), adolescent (12 to <18 years), and adult (≥18 years). We used unadjusted and adjusted logistic regression to test if age group was associated with vital signs documentation, reporting of Glasgow Coma Scale and pain scale after trauma, and recording of oxygen saturation and breath sounds in respiratory complaints, using adults as the reference group.
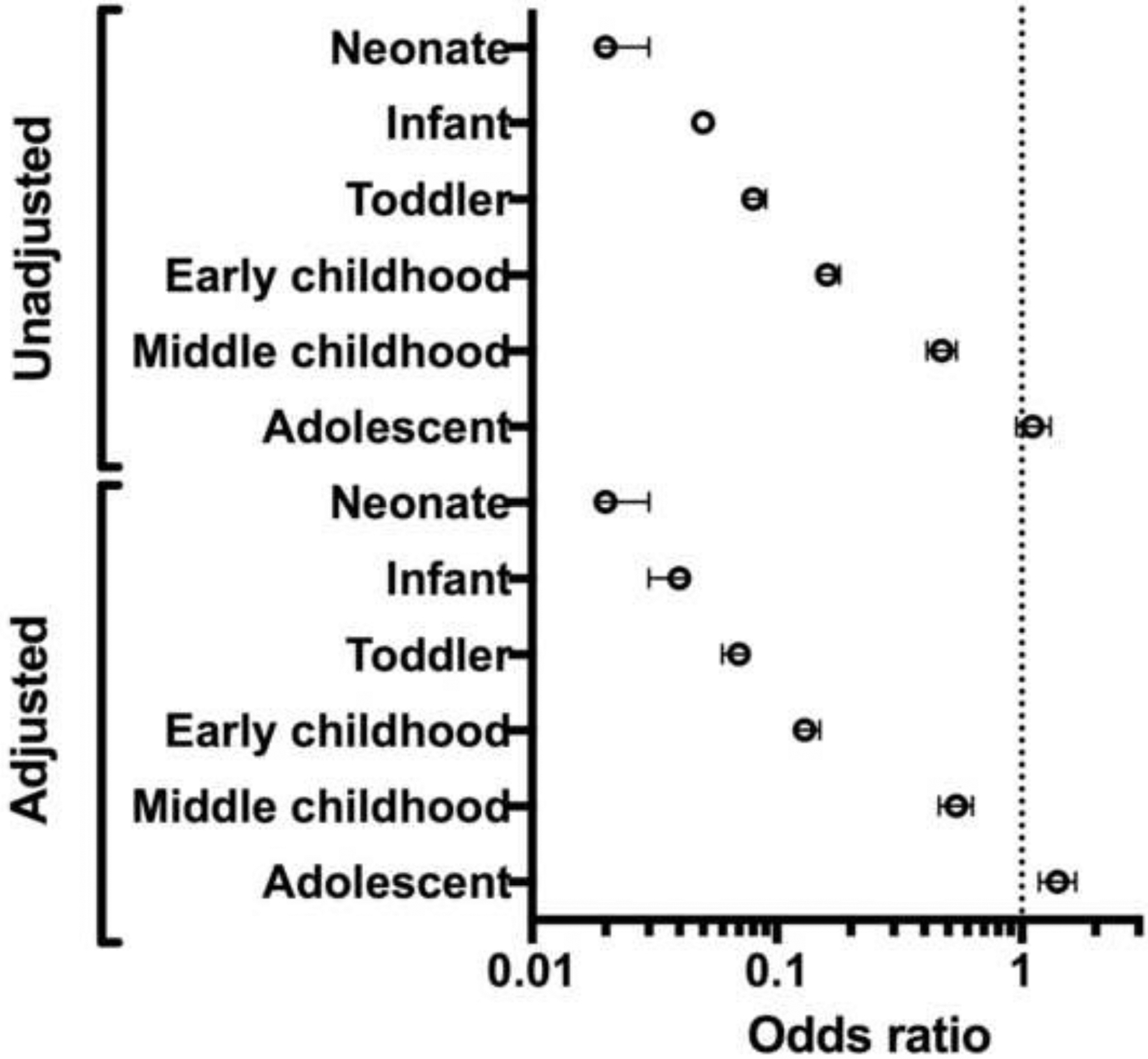
Results: In total, 371 746 cases (21 883 pediatric, 5.9%) were included. In adjusted analysis, most pediatric categories had reduced odds of complete vitals documentation (percent, OR, 95% CI): neonates (49.6%, 0.02, 0.02-0.03), infants (68.2%, 0.04, 0.03-0.04), toddlers (78.1%, 0.07, 0.06-0.07), early childhood (87.4%, 0.13, 0.12-0.15), and middle childhood (95.3%, 0.54, 0.46-0.63). Pain score documentation was lower in children after trauma (OR 0.80, 95%CI 0.76-0.85), and oxygen saturation documentation was lower in children with respiratory complaints (OR 0.20, 95%CI 0.18-0.25).
Conclusions: Pediatric patients were at increased risk of lacking vital signs documentation during prehospital care. This represents a critical area for education and quality improvement.
Keywords: emergency medical services; prehospital medicine.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Tsai A, Kallsen G. Epidemiology of pediatric prehospital care. Ann Emerg Med. 1987;16:284–92. - PubMed
-
- Seidel JS, Hornbein M, Yoshiyama K, Kuznets D, Finklestein JZ, St Geme JW Jr.. Emergency medical services and the pediatric patient: are the needs being met? Pediatrics. 1984;73:769–72. - PubMed
-
- Brown SA, Hayden TC, Randell KA, Rappaport L, Stevenson MD, Kim IK. Improving Pediatric Education for Emergency Medical Services Providers: A Qualitative Study. Prehosp Disaster Med. 2017;32:20–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
