

Diagnostic criteria for camptocormia in Parkinson's disease: A consensus-based proposal
- PMID: 29759930
- PMCID: PMC7293065
- DOI: 10.1016/j.parkreldis.2018.04.033
Diagnostic criteria for camptocormia in Parkinson's disease: A consensus-based proposal
Abstract
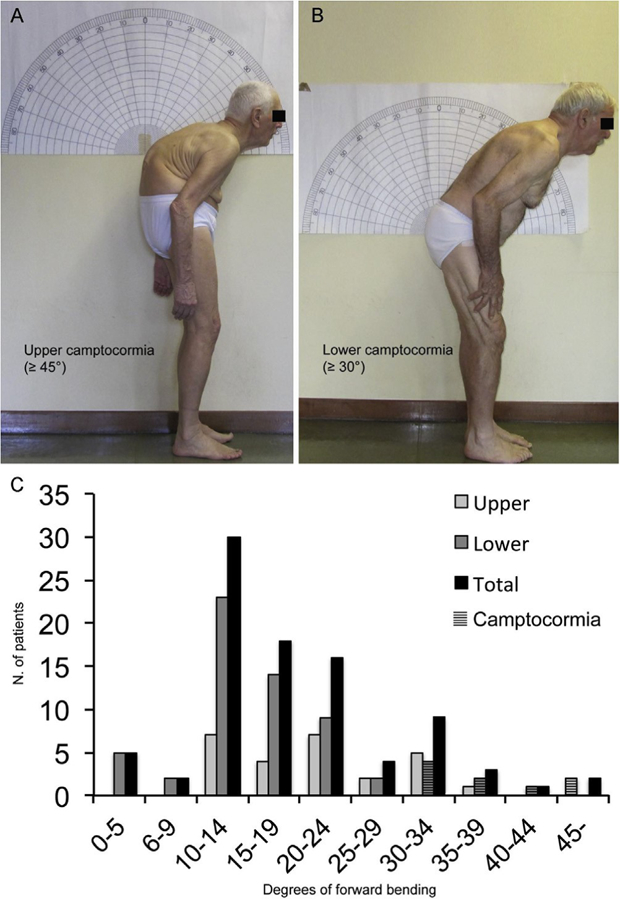
Introduction: Camptocormia is defined as an involuntary, marked flexion of the thoracolumbar spine appearing during standing or walking and resolving in the supine position or when leaning against a wall. However, there is no established agreement on the minimum degree of forward flexion needed to diagnose camptocormia. Likewise, the current definition does not categorize camptocormia on the basis of the bending fulcrum.
Methods: We performed a survey among movement disorders experts to identify camptocormia using images of patients with variable degrees and types of forward trunk flexion by fulcrum (upper and lower fulcra). We tested the subsequently generated diagnostic criteria in a sample of 131 consecutive patients referred for evaluation of postural abnormalities.
Results: Experts reached full consensus on lower camptocormia (L1-Sacrum, hip flexion) with a bending angle ≥30° and upper camptocormia (C7 to T12-L1) with a bending angle ≥45°. This definition detected camptocormia in 9/131 consecutive PD patients (2 upper/7 lower) but excluded camptocormia in 71 patients considered to have camptocormia by the referring neurologist.
Conclusions: Camptocormia can be defined as "an involuntary flexion of the spine appearing during standing or walking and resolving in the supine position of at least 30° at the lumbar fulcrum (L1-Sacrum, hip flexion, i.e. lower camptocormia) and/or at least 45° at the thoracic fulcrum (C7 to T12-L1, i.e. upper camptocormia)". Strict criteria for camptocormia are met by 7% of patients with abnormal posture. The ascertainment of upper and lower camptocormia subtypes could improve the validity of epidemiological studies and assist future therapeutic trials.
Keywords: Back pain; Bent spine syndrome; Camptocormia; Postural abnormalities; Stooped posture.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures
References
-
- Doherty KM, van de Warrenburg BP, Peralta MC, Silveira-Moriyama L, Azulay JP, Gershanik OS, Bloem BR, Postural deformities in Parkinson’s disease, Lancet Neurol 10 (2011) 538–549. - PubMed
-
- Ashour R, Jankovic J, Joint and skeletal deformities in Parkinson’s disease, multiple system atrophy, and progressive supranuclear palsy, Mov. Disord 21 (2006) 1856–1863. - PubMed
-
- Tiple D, Fabbrini G, Colosimo C, Ottaviani D, Camerota F, Defazio G, Berardelli A, Camptocormia in Parkinson disease: an epidemiological and clinical study, J. Neurol. Neurosurg. Psychiatry 80 (2009) 145–148. - PubMed
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
