

Pathways and mechanisms linking dietary components to cardiometabolic disease: thinking beyond calories
- PMID: 29761610
- PMCID: PMC6530989
- DOI: 10.1111/obr.12699
Pathways and mechanisms linking dietary components to cardiometabolic disease: thinking beyond calories
Abstract
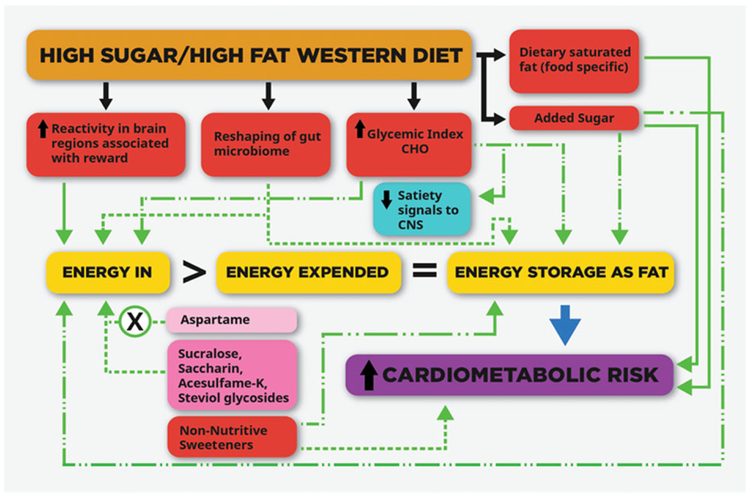
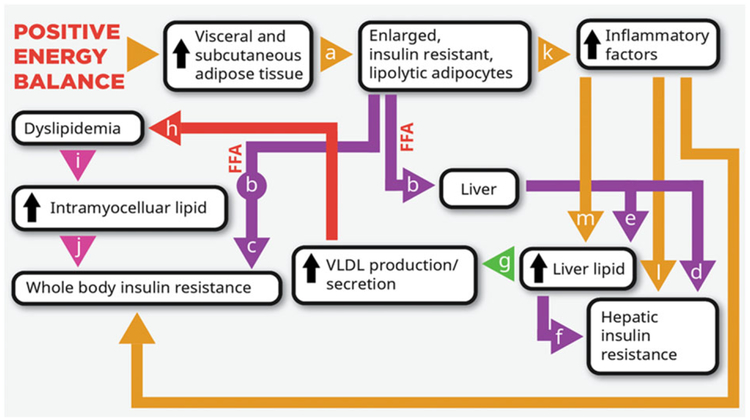
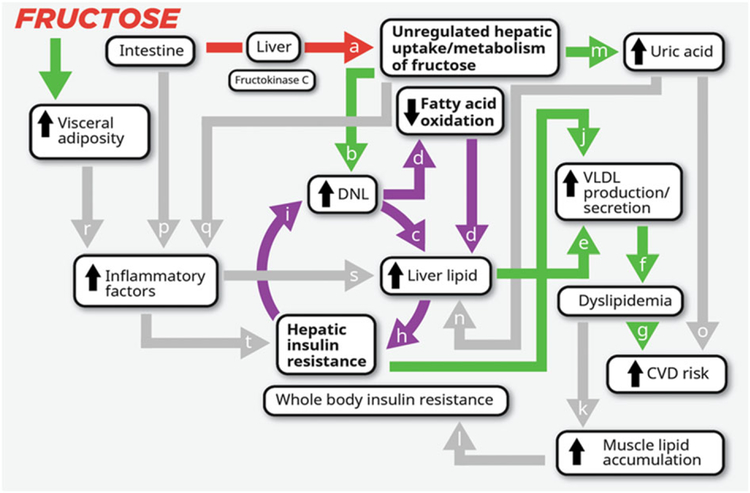
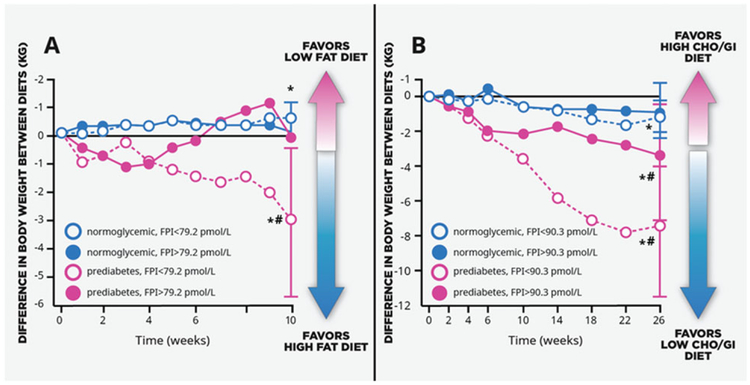
Calories from any food have the potential to increase risk for obesity and cardiometabolic disease because all calories can directly contribute to positive energy balance and fat gain. However, various dietary components or patterns may promote obesity and cardiometabolic disease by additional mechanisms that are not mediated solely by caloric content. Researchers explored this topic at the 2017 CrossFit Foundation Academic Conference 'Diet and Cardiometabolic Health - Beyond Calories', and this paper summarizes the presentations and follow-up discussions. Regarding the health effects of dietary fat, sugar and non-nutritive sweeteners, it is concluded that food-specific saturated fatty acids and sugar-sweetened beverages promote cardiometabolic diseases by mechanisms that are additional to their contribution of calories to positive energy balance and that aspartame does not promote weight gain. The challenges involved in conducting and interpreting clinical nutritional research, which preclude more extensive conclusions, are detailed. Emerging research is presented exploring the possibility that responses to certain dietary components/patterns are influenced by the metabolic status, developmental period or genotype of the individual; by the responsiveness of brain regions associated with reward to food cues; or by the microbiome. More research regarding these potential 'beyond calories' mechanisms may lead to new strategies for attenuating the obesity crisis.
Keywords: Cardiometabolic disease; dietary fat; dietary sugar; obesity.
© 2018 The Authors. Obesity Reviews published by John Wiley & Sons Ltd on behalf of World Obesity Federation.
Conflict of interest statement
Conflict of interest statement
The following authors have no conflicts of interest to report: Drs Schmidt, Turnbaugh and Bray.
The following authors acknowledge these conflicts of interest.
Dr Stanhope received honoraria from the CrossFit Foundation for serving as a Conference Academic Organizer and for writing the manuscript.
Dr Goran received honorarium from the CrossFit Foundation for serving on the Advisory Committee and travel reimbursement from the CrossFit Foundation for attending the conference in July 2017.
Drs Bosy-Westphal, King, Schwarz, Sylvetsky, Gardner, Mason, Rosenbaum and Allister-Price and Ms Sigala received travel reimbursement from the CrossFit Foundation for attending the conference in July 2017.
Dr Malik received travel reimbursement from the CrossFit Foundation for attending the conference in July 2017. She was paid for consulting services by the City of San Francisco for litigation related to health warning labels of soda and is on a pro bono retainer to The Center for Science in the Public Interest for expert support in litigation related to sugar-sweetened beverages.
Dr Havel received travel reimbursement from the CrossFit Foundation for attending the conference in July 2017. He has received research grants from Bristol Myers Squibb and Arrowhead Pharmaceuticals.
Dr Stice received travel reimbursement from the CrossFit Foundation for attending the conference in July 2017. His institution has received research funding from Crave Crush, and he has received reimbursement for travel from Crave Crush.
Dr Ravussin received travel reimbursement from the CrossFit Foundation for attending the conference in July 2017. He serves on the Scientific Advisory Board to the Nutrilite Health Institute with Amway and for the Institute of Cardiometabolism and Nutrition in Paris, France; has a consultant contract with Janssen and with Nutrilite Health Institute with Amway; gives lectures at the Open Academy in Venice; and is a lecturer/advisor for the Center for Medical Weight Loss. He has received research grants or unrestricted gifts from Amway, Nestle, the Nutrition Science Initiative, Novartis, Sanofi-Aventis, Weight Watchers and Ethicon Surgery. He has a patent for ‘Night Moderate Hypoxia to Treat Insulin Resistance and Cardiometabolic Syndrome’.
Dr Welsh received travel reimbursement from the CrossFit Foundation for attending the conference in July 2017. She received payment from the Sugar Foundation for an analysis and presentation on sugar consumption in toddlers.
Dr Greenwood received honorarium for serving as Chairperson of the manuscript planning meeting and travel reimbursement from the CrossFit Foundation for attending the conference in July 2017.
Dr Astrup received honorarium from CrossFit Foundation for serving on the Advisory Committee and travel reimbursement from CrossFit Foundation for attending the conference in July 2017. He reports personal fees from Dutch Beer Institute, NL; Feast Kitchen A/S, Denmark; Groupe Éthique et Santé, France; McCain Foods Limited, USA; Nestlé Research Center, Switzerland; Weight Watchers, USA; BioCare Copenhagen, Zaluvida, Switzerland; Basic Research, USA; Beachbody, USA; Danish Agriculture & Food Council, Novo Nordisk, Denmark; Pfizer, Germany; Saniona, Denmark; Sanofi-Aventis, Germany; S-Biotek, Denmark; Scandinavian Airlines System, Denmark; and Tetra Pak, Sweden; personal fees and other from Gelesis, USA; grants from Arla Foods, DK; Danish Dairy Research Council; and Gelesis, USA outside the submitted work. In addition, Dr Astrup has a patents pending to the University of Copenhagen ‘Methods of inducing weight loss, treating obesity and preventing weight gain’ (licensee Gelesis, USA) and ‘Biomarkers for predicting degree of weight loss’ (licensee Nestec SA, CH), and he is a co-inventor of a number of other patents owned by the University in accordance with Danish law. Astrup receives royalties for the books
Dr Krauss received honorarium from CrossFit Foundation for serving on the Advisory Committee and travel reimbursement from CrossFit Foundation for attending the conference in July 2017. He has received payment for services on the Scientific Advisory Board of Virta Health and from Quest Diagnostics for services on speakers bureau. He has received research grants from the Almond Board of California and The Dairy Research Institute. He has a patent on lipoprotein particle analysis.
Figures
References
-
- Rodriguez-Ramirez S, Mundo-Rosas V, Garcia-Guerra A, Shamah-Levy T. Dietary patterns are associated with overweight and obesity in Mexican school-age children. Arch Latinoam Nutr 2011; 61: 270–278. - PubMed
-
- Naja F, Nasreddine L, Itani L et al. Dietary patterns and their association with obesity and sociodemographic factors in a national sample of Lebanese adults. Public Health Nutr 2011; 14: 1570–1578. - PubMed
-
- Jensen MD, Ryan DH, Apovian CM et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014; 129: S102–S138. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
