

Clinical indications associated with opioid initiation for pain management in Ontario, Canada: a population-based cohort study
- PMID: 29762260
- PMCID: PMC6085129
- DOI: 10.1097/j.pain.0000000000001242
Clinical indications associated with opioid initiation for pain management in Ontario, Canada: a population-based cohort study
Abstract
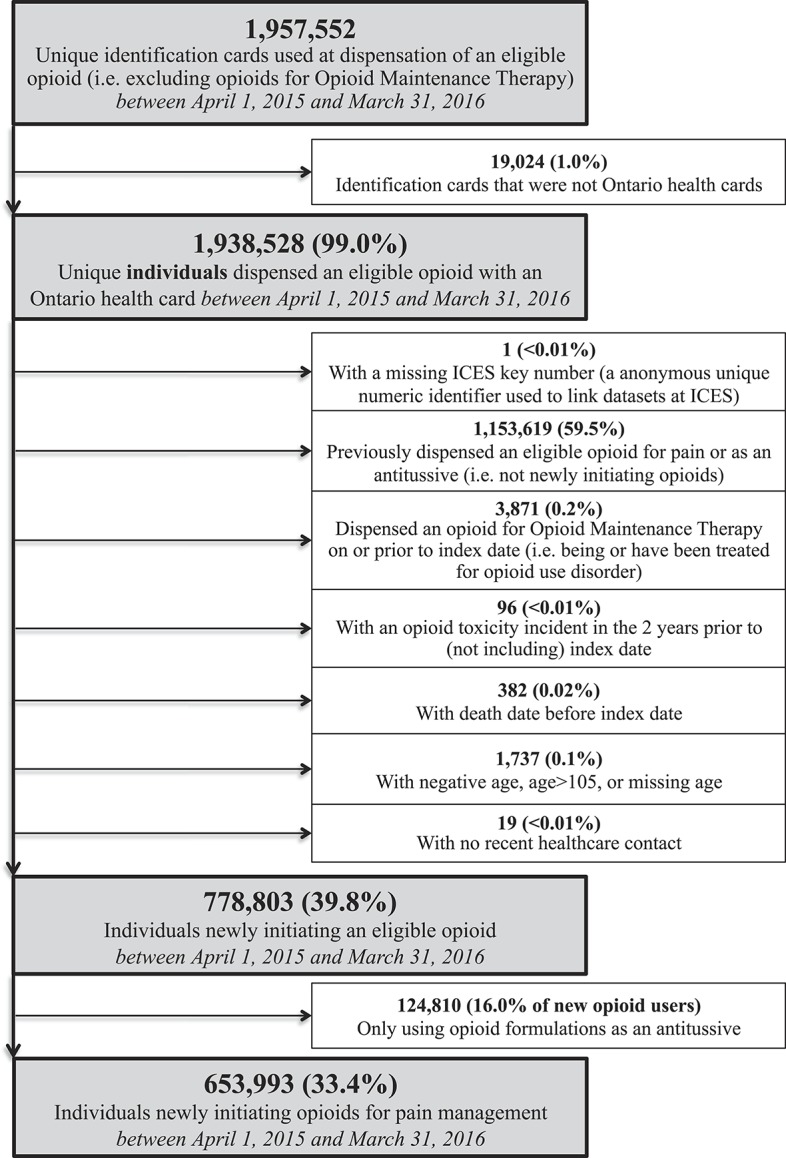
Concerns over prescription opioids contributing to high levels of opioid use disorder and overdose have led policymakers and clinicians to seek means to reduce inappropriate and high-dose initial prescriptions. To inform such efforts, we sought to describe the clinical indications associated with opioid initiation and the characteristics of the initial prescriptions and patients through a retrospective population-based cohort study. Our cohort included Ontarians initiating prescription opioids for pain management between April 1, 2015, and March 31, 2016. We identified the apparent clinical indication for opioid initiation by linking prescription drug claims to procedural and diagnostic information on health service records on the day of, and 5 days preceding prescription. Outcomes included initial opioid type, prescription duration, and daily dose (in milligram morphine equivalents), stratified either by indication or indication cluster. Among 653,993 individuals, we successfully classified 575,512 (88.0%) people initiating opioids into 23 clinical indications in 6 clusters: dental (23.2%); postsurgical (17.4%); musculoskeletal (12.0%); trauma (11.2%); cancer/palliative care (6.5%); and other less frequent indications (17.7%). Individuals with postsurgical pain received the highest daily doses (40.5% with greater than 50 milligram morphine equivalent), and those with musculoskeletal pain received more initial prescriptions with a duration exceeding 7 days (34.2%). Opioids are initiated for a wide range of indications with varying doses and durations; yet, those who initiated opioids for postsurgical and musculoskeletal pain received the greatest doses and durations of therapy, respectively. These findings may help tailor and prioritize efforts to promote more appropriate opioid prescribing.
Conflict of interest statement
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
References
-
- Busse JW, Craigie S, Juurlink DN, Buckley DN, Wang L, Couban RJ, Agoritsas T, Akl EA, Carrasco-Labra A, Cooper L, Cull C, da Costa BR, Frank JW, Grant G, Iorio A, Persaud N, Stern S, Tugwell P, Vandvik PO, Guyatt GH. Guideline for opioid therapy and chronic noncancer pain. CMAJ 2017;189:E659–66. - PMC - PubMed
-
- Canadian Institute for Health Information. The CIHI data quality framework. Ottawa: CIHI, 2009.
-
- Casucci G, Cevoli S. Controversies in migraine treatment: opioids should be avoided. Neurol Sci 2013;34(suppl 1):S125–128. - PubMed
-
- Clarke J. “Difficulty accessing health care services in Canada.” Health at a Glance. Ottawa, ON, Canada: Statistics Canada catalogue no. 82-624-X; 2016.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
