

Practice and outcomes of neonatal resuscitation for newborns with birth asphyxia at Kakamega County General Hospital, Kenya: a direct observation study
- PMID: 29764391
- PMCID: PMC5953400
- DOI: 10.1186/s12887-018-1127-6
Practice and outcomes of neonatal resuscitation for newborns with birth asphyxia at Kakamega County General Hospital, Kenya: a direct observation study
Abstract
Background: About three - quarters of all neonatal deaths occur during the first week of life, with over half of these occurring within the first 24 h after birth. The first minutes after birth are critical to reducing neonatal mortality. Successful neonatal resuscitation (NR) has the potential to prevent these perinatal mortalities related to birth asphyxia. This study described the practice of NR and outcomes of newborns with birth asphyxia in a busy referral hospital.
Methods: Direct observations of 138 NRs by 28 healthcare providers (HCPs) were conducted using a predetermined checklist adapted from the national pediatric resuscitation protocol. Descriptive statistics were computed and chi - square tests were used to test associations between the newborn outcome at 1 h and the NR processes for the observed newborns. Logistic regression models assessed the relationship between the survival status at 1 h versus the NR processes and newborn characteristics.
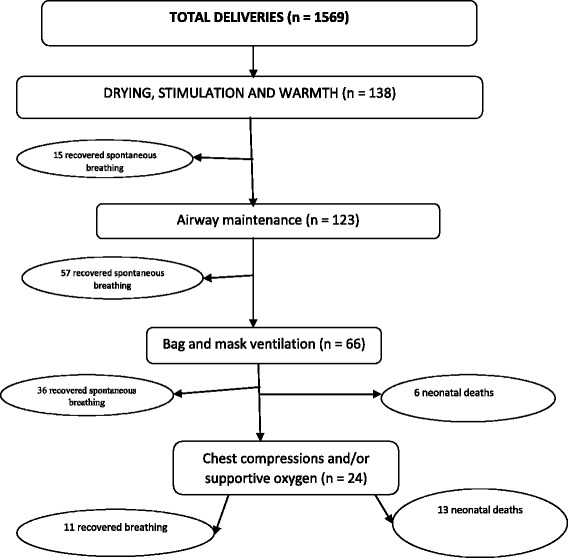
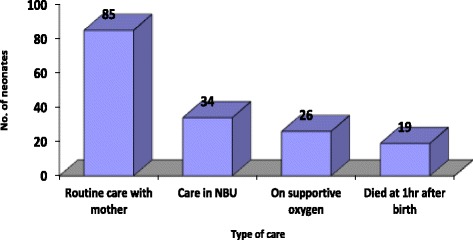
Results: Nurses performed 72.5% of the NRs. A warm environment was maintained in 71% of the resuscitations. Airway was checked for almost all newborns (98%) who did not initiate spontaneous breathing after stimulation. However, only 40% of newborns were correctly cared for in case of meconium presence in airway. Bag and mask ventilation (BMV) was initiated in 100% of newborns who did not respond to stimulation and airway maintenance. About 86.2% of resuscitated newborns survived after 1 h. Removing wet cloth (P = 0.035, OR = 2.90, CI = 1.08-7.76), keeping baby warm (P = 0.018, OR = 3.30, CI = 1.22-8.88), meconium in airway (P = 0.042, OR = 0.34, CI = 0.12-0.96) and gestation age (P = 0.007, OR = 1.38, CI = 1.10-1.75) were associated with newborn outcome at 1 h.
Conclusions: Mentorship and regular cost - effective NR trainings with focus on maintaining the warm chain during NR, airway maintenance in meconium presence, BMV and care for premature babies are needed for HCPs providing NR.
Keywords: Birth asphyxia; Kenya; Neonatal resuscitation; Newborn.
Conflict of interest statement
Ethics approval and consent to participate
The study protocols were approved by the Makerere University, School of Health Sciences Institutional Review Board (IRB) (SHSREC REF: 2015–028), Moi University/Moi Teaching and Referral Hospital (MTRH) Institutional Research and Ethics Committee (IREC) (FAN: IREC 1608 and the Kakamega County General Hospital Ethics and Research Committee (ERC no. 9/04/2016. Written informed consent was obtained from the HCPs prior to inclusion in the study. Verbal informed consent was secured by the research assistants from both low and high risk mothers during the first stage of labor as it is difficult to predict that the baby would need help to breathe immediately after birth. Later, all those who met the criteria were observed irrespective of the mode of delivery. There was apprehension on the side of HCPs on repercussions in case of identification of incorrect practices or poor skills. However, they were assured that the records would not bear any identification apart from the anonymous study code and strict observation of confidentiality at all levels of the study was maintained.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- WHO. Guidelines on basic newborn resuscitation: World Health Organization; 2012. - PubMed
-
- Bang A, Bellad R, Gisore P, Hibberd P, Patel A, Goudar S, et al. Implementation and evaluation of the helping babies breathe curriculum in three resource limited settings: does helping babies breathe save lives? A study protocol. BMC pregnancy and childbirth. 2014;14(1):116. doi: 10.1186/1471-2393-14-116. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
