

Gestational diabetes is associated with change in the gut microbiota composition in third trimester of pregnancy and postpartum
- PMID: 29764499
- PMCID: PMC5952429
- DOI: 10.1186/s40168-018-0472-x
Gestational diabetes is associated with change in the gut microbiota composition in third trimester of pregnancy and postpartum
Abstract
Background: Imbalances of gut microbiota composition are linked to a range of metabolic perturbations. In the present study, we examined the gut microbiota of women with gestational diabetes mellitus (GDM) and normoglycaemic pregnant women in late pregnancy and about 8 months postpartum.
Methods: Gut microbiota profiles of women with GDM (n = 50) and healthy (n = 157) pregnant women in the third trimester and 8 months postpartum were assessed by 16S rRNA gene amplicon sequencing of the V1-V2 region. Insulin and glucose homeostasis were evaluated by a 75 g 2-h oral glucose tolerance test during and after pregnancy.
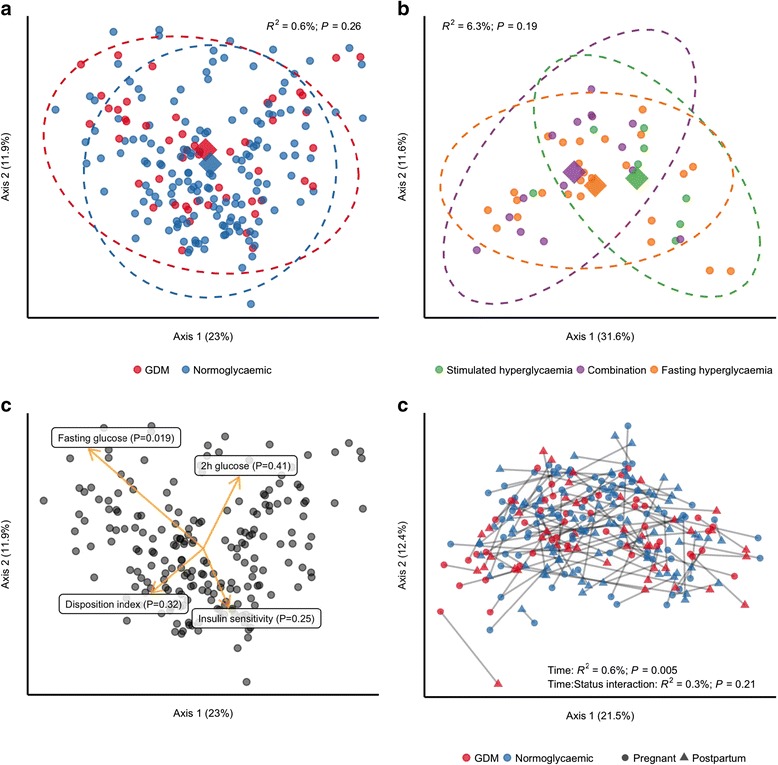
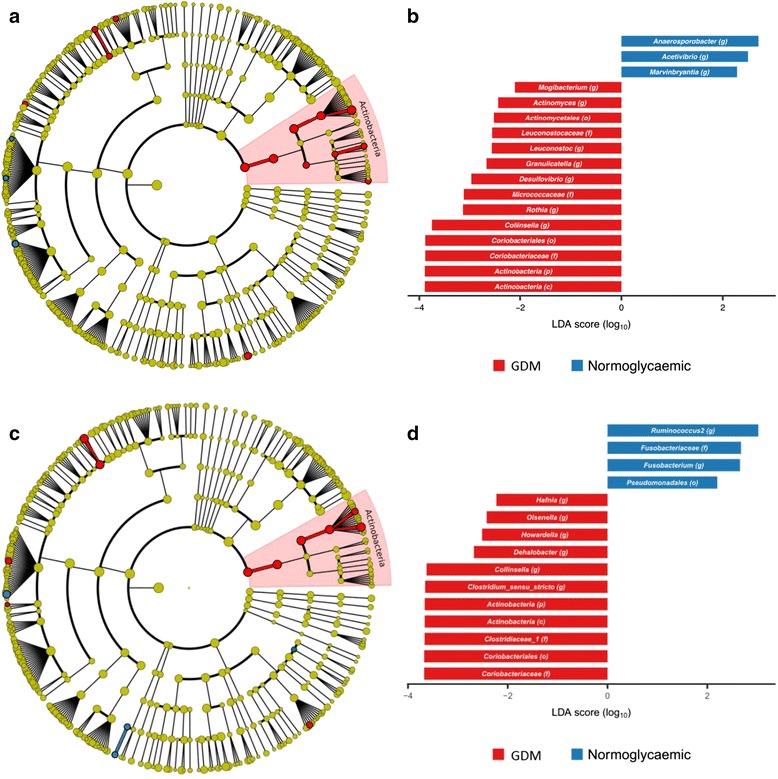
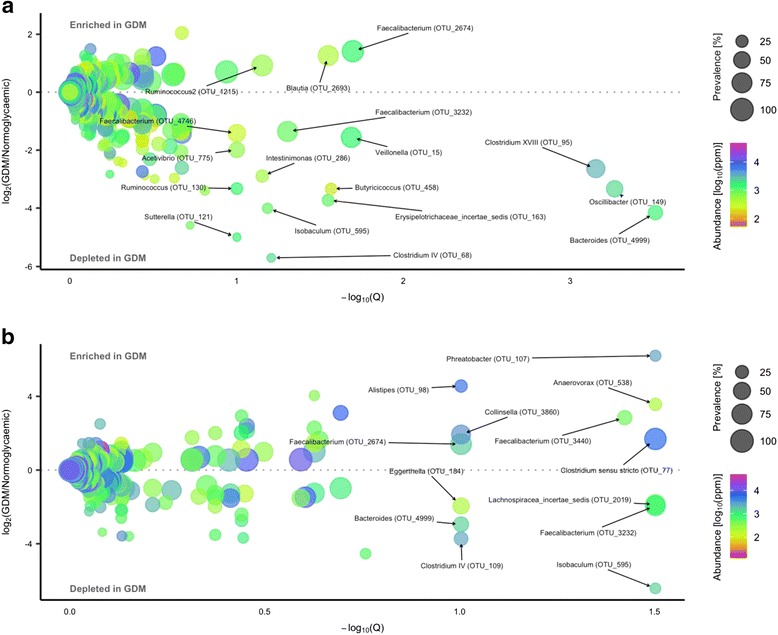
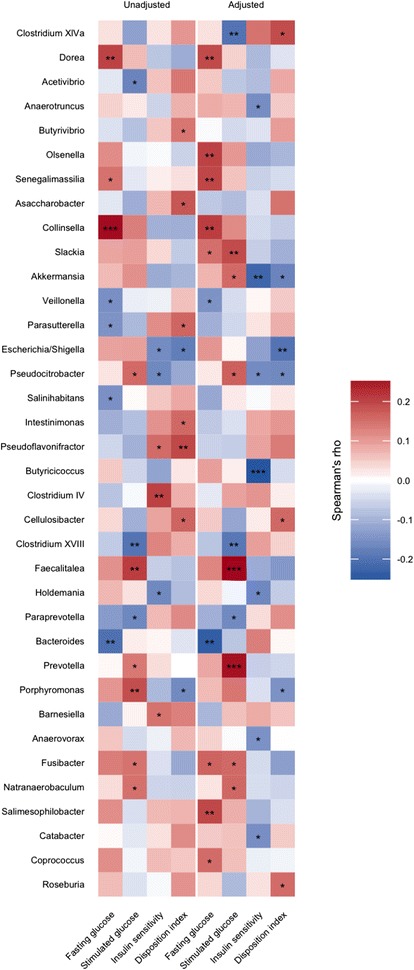
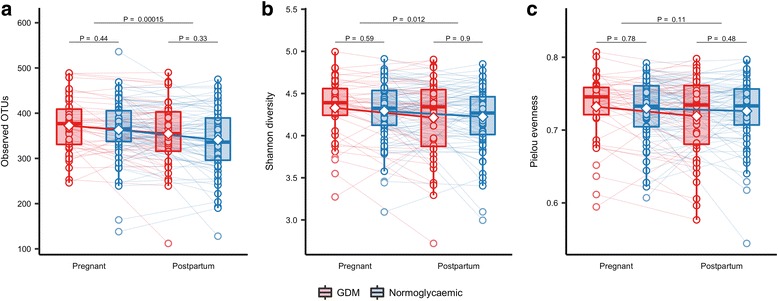
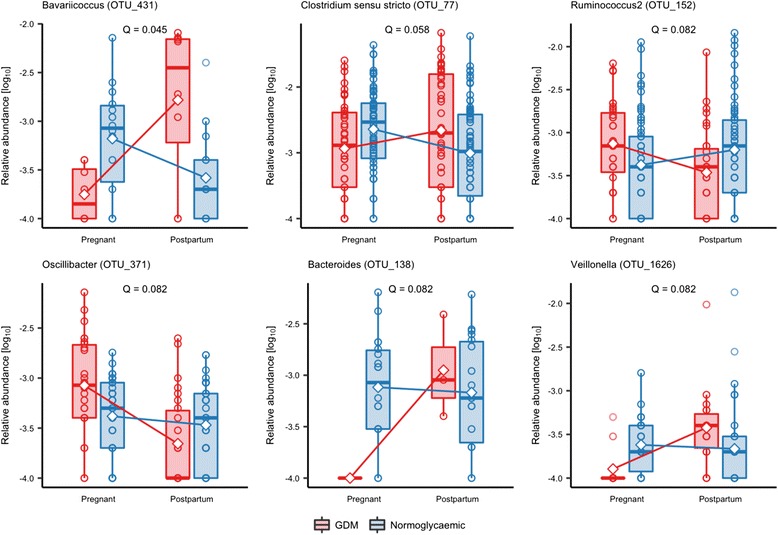
Results: Gut microbiota of women with GDM was aberrant at multiple levels, including phylum and genus levels, compared with normoglycaemic pregnant women. Actinobacteria at phylum level and Collinsella, Rothia and Desulfovibrio at genus level had a higher abundance in the GDM cohort. Difference in abundance of 17 species-level operational taxonomic units (OTUs) during pregnancy was associated with GDM. After adjustment for pre-pregnancy body mass index (BMI), 5 of the 17 OTUs showed differential abundance in the GDM cohort compared with the normoglycaemic pregnant women with enrichment of species annotated to Faecalibacterium and Anaerotruncus and depletion of species annotated to Clostridium (sensu stricto) and to Veillonella. OTUs assigned to Akkermansia were associated with lower insulin sensitivity while Christensenella OTUs were associated with higher fasting plasma glucose concentration. OTU richness and Shannon index decreased from late pregnancy to postpartum regardless of metabolic status. About 8 months after delivery, the microbiota of women with previous GDM was still characterised by an aberrant composition. Thirteen OTUs were differentially abundant in women with previous GDM compared with women with previous normoglycaemic pregnancy.
Conclusion: GDM diagnosed in the third trimester of pregnancy is associated with a disrupted gut microbiota composition compared with normoglycaemic pregnant women, and 8 months after pregnancy, differences in the gut microbiota signatures are still detectable. The gut microbiota composition of women with GDM, both during and after pregnancy, resembles the aberrant microbiota composition reported in non-pregnant individuals with type 2 diabetes and associated intermediary metabolic traits.
Keywords: Bacterial species; Body mass index; Gestational diabetes; Gestational hyperglycaemia; Glycaemic traits; Gut microbiota; Pregnancy.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Ethical Committees of the Capital Region of Denmark (Protocol #H-4-2013-10) and conducted in accordance with the principles of the Declaration of Helsinki II. Written informed consent was obtained from all participants.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Lain KY, Catalano P. Metabolic changes in pregnancy. Clinical Obstet Gynecol n.d. 2007:938–48. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
