

Neural predisposing factors of postoperative delirium in elderly patients with femoral neck fracture
- PMID: 29765105
- PMCID: PMC5954080
- DOI: 10.1038/s41598-018-26030-2
Neural predisposing factors of postoperative delirium in elderly patients with femoral neck fracture
Abstract
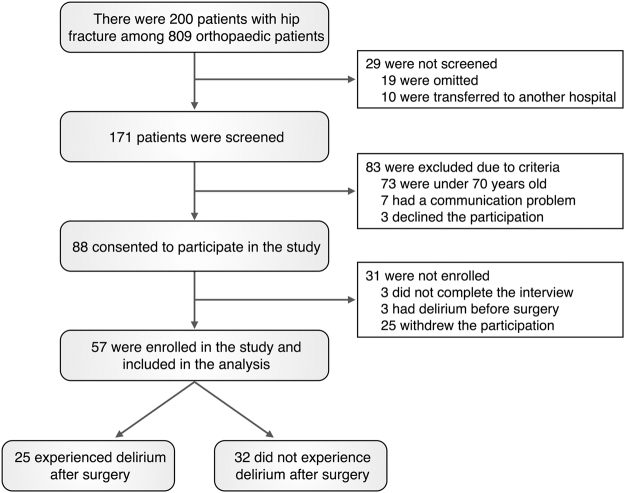
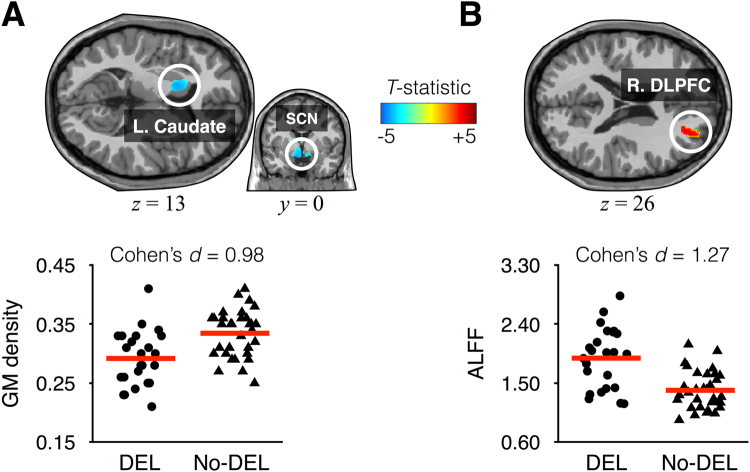
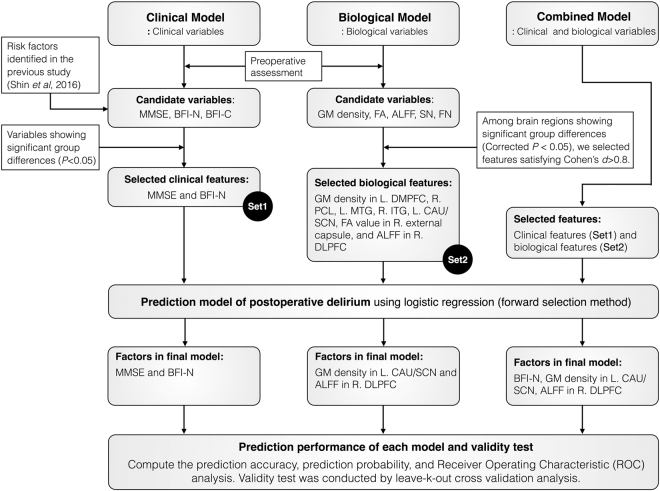
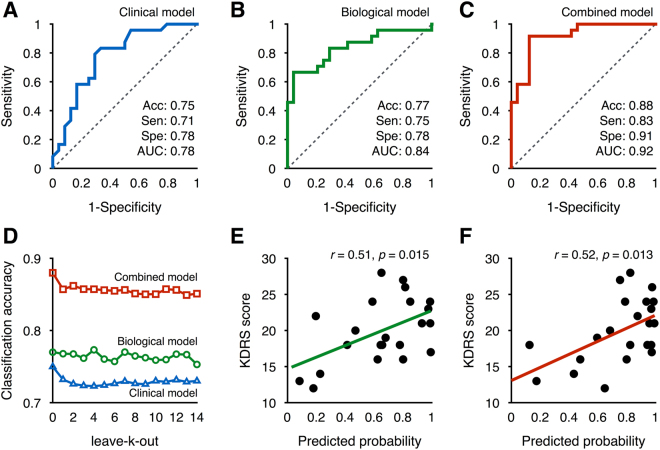
Elderly adults are more likely to develop delirium after major surgery, but there is limited knowledge of the vulnerability for postoperative delirium. In this study, we aimed to identify neural predisposing factors for postoperative delirium and develop a prediction model for estimating an individual's probability of postoperative delirium. Among 57 elderly participants with femoral neck fracture, 25 patients developed postoperative delirium and 32 patients did not. We preoperatively obtained data for clinical assessments, anatomical MRI, and resting-state functional MRI. Then we evaluated gray matter (GM) density, fractional anisotropy, and the amplitude of low-frequency fluctuation (ALFF), and conducted a group-level inference. The prediction models were developed to estimate an individual's probability using logistic regression. The group-level analysis revealed that neuroticism score, ALFF in the dorsolateral prefrontal cortex, and GM density in the caudate/suprachiasmatic nucleus were predisposing factors. The prediction model with these factors showed a correct classification rate of 86% using a leave-one-out cross-validation. The predicted probability computed from the logistic model was significantly correlated with delirium severity. These results suggest that the three components are the most important predisposing factors for postoperative delirium, and our prediction model may reflect the core pathophysiology in estimating the probability of postoperative delirium.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Delirium before and after operation for femoral neck fracture.J Am Geriatr Soc. 2001 Oct;49(10):1335-40. doi: 10.1046/j.1532-5415.2001.49261.x. J Am Geriatr Soc. 2001. PMID: 11890492
-
A Decrease in the Volume of Gray Matter as a Risk Factor for Postoperative Delirium Revealed by an Atlas-based Method.Am J Geriatr Psychiatry. 2016 Jul;24(7):528-36. doi: 10.1016/j.jagp.2015.09.002. Epub 2015 Sep 14. Am J Geriatr Psychiatry. 2016. PMID: 26654288
-
[Postoperative complications after femoral neck fracture in advanced elderly patients].Masui. 2008 Feb;57(2):163-6. Masui. 2008. PMID: 18277562 Japanese.
-
Postoperative delirium in the elderly surgical patient.Anesthesiol Clin. 2009 Sep;27(3):451-64, table of contents. doi: 10.1016/j.anclin.2009.07.009. Anesthesiol Clin. 2009. PMID: 19825486 Review.
-
Pathogenesis of and management strategies for postoperative delirium after hip fracture: a review.Acta Orthop Scand. 2004 Aug;75(4):378-89. doi: 10.1080/00016470410001123. Acta Orthop Scand. 2004. PMID: 15370579 Review.
Cited by
-
Treatment effect of elastic intramedullary nail reduction and fixation on children with femoral neck fractures.Am J Transl Res. 2021 Oct 15;13(10):12083-12089. eCollection 2021. Am J Transl Res. 2021. PMID: 34786145 Free PMC article.
-
Predilection for Perplexion: Preoperative microstructural damage is linked to postoperative delirium.medRxiv [Preprint]. 2025 Jan 9:2025.01.08.24319243. doi: 10.1101/2025.01.08.24319243. medRxiv. 2025. PMID: 39830255 Free PMC article. Preprint.
-
The impact of circulatory arrest with selective antegrade cerebral perfusion on brain functional connectivity and postoperative cognitive function.Sci Rep. 2023 Aug 23;13(1):13803. doi: 10.1038/s41598-023-40726-0. Sci Rep. 2023. PMID: 37612347 Free PMC article.
-
The Effects of Transcranial Direct Current Stimulation on the Cognitive and Behavioral Changes After Electrode Implantation Surgery in Rats.Front Psychiatry. 2019 May 7;10:291. doi: 10.3389/fpsyt.2019.00291. eCollection 2019. Front Psychiatry. 2019. PMID: 31156472 Free PMC article.
-
Assessment and report of individual symptoms in studies of delirium in postoperative populations: a systematic review.Age Ageing. 2024 Apr 1;53(4):afae077. doi: 10.1093/ageing/afae077. Age Ageing. 2024. PMID: 38640126 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
