

Post-stroke Intranasal (+)-Naloxone Delivery Reduces Microglial Activation and Improves Behavioral Recovery from Ischemic Injury
- PMID: 29766045
- PMCID: PMC5952324
- DOI: 10.1523/ENEURO.0395-17.2018
Post-stroke Intranasal (+)-Naloxone Delivery Reduces Microglial Activation and Improves Behavioral Recovery from Ischemic Injury
Abstract
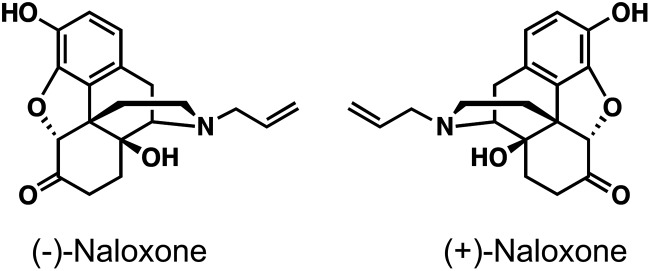
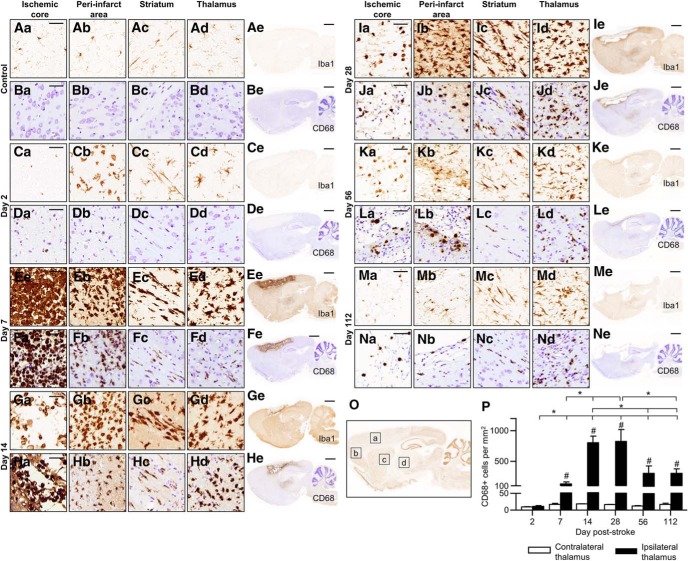
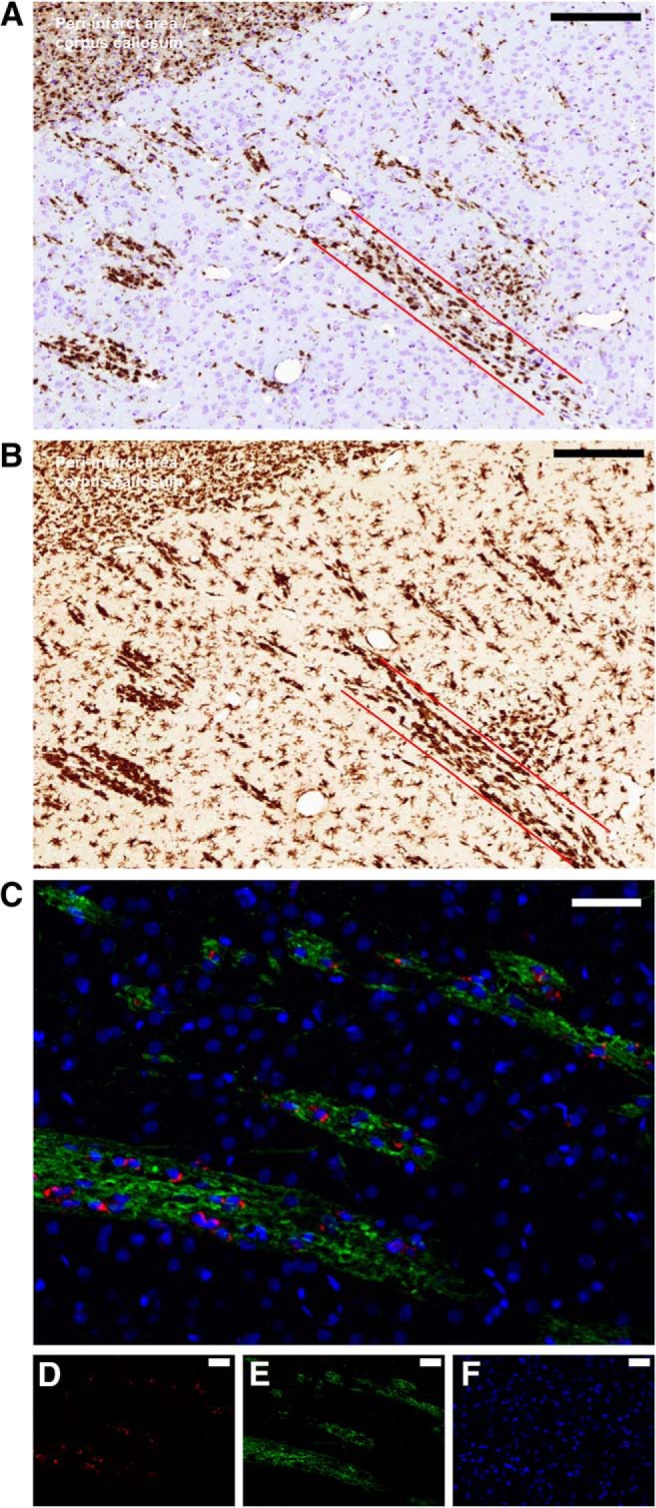
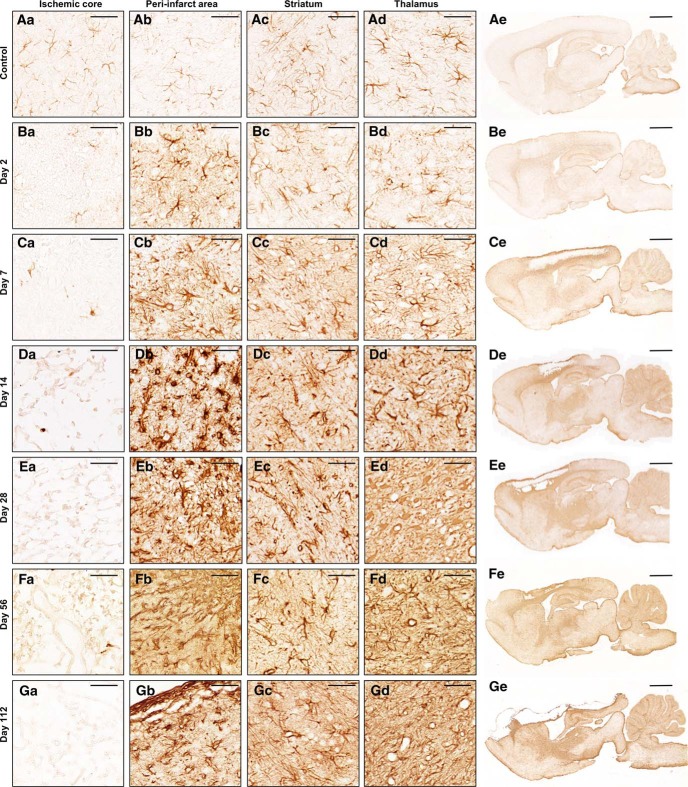
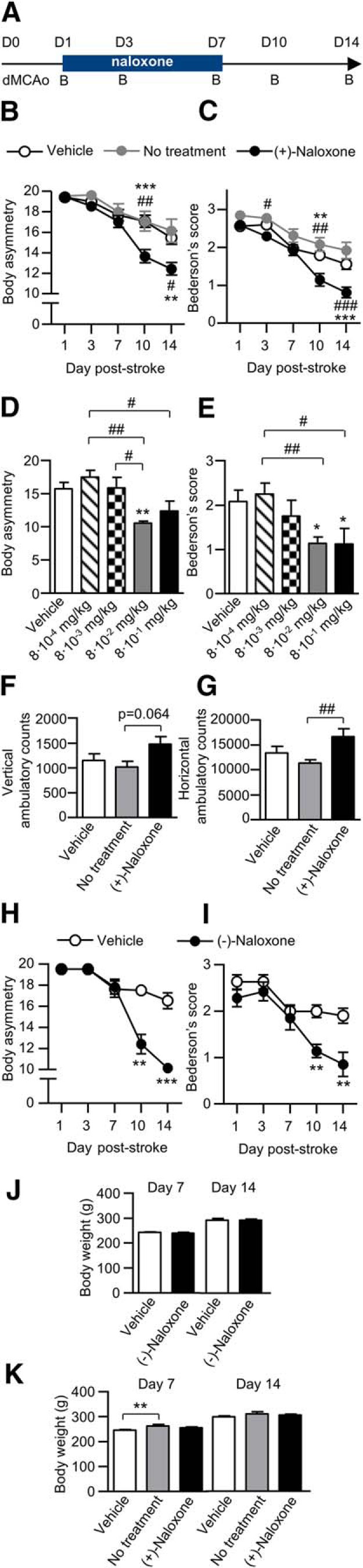
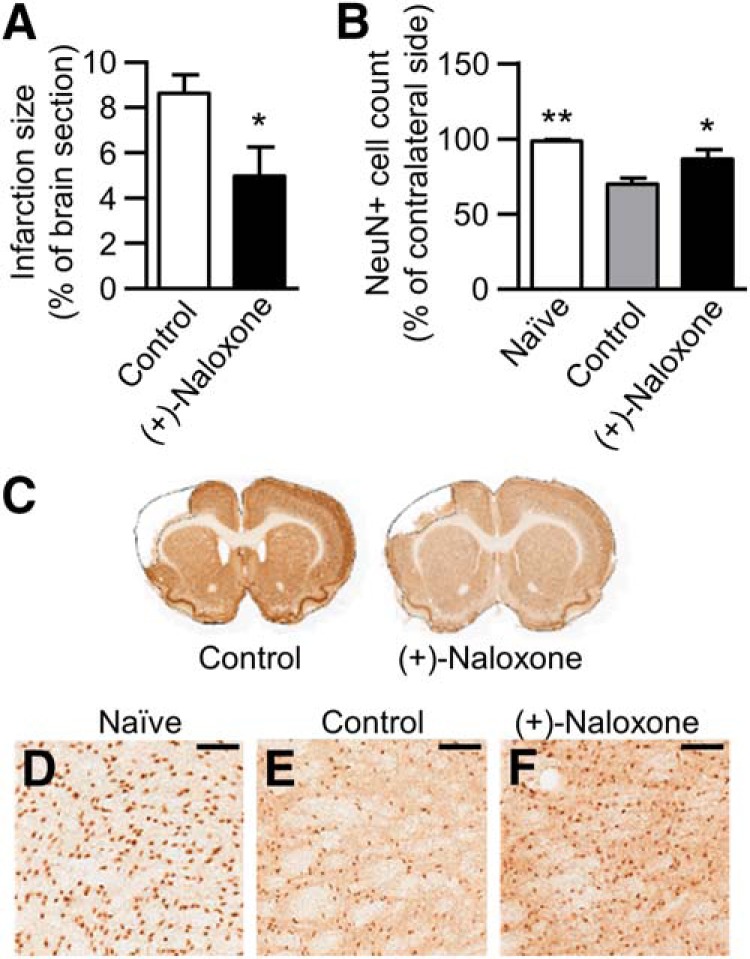
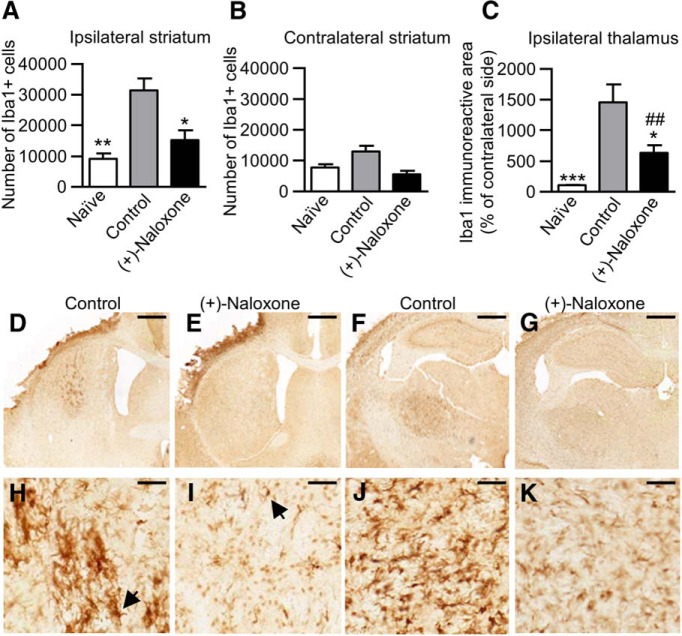
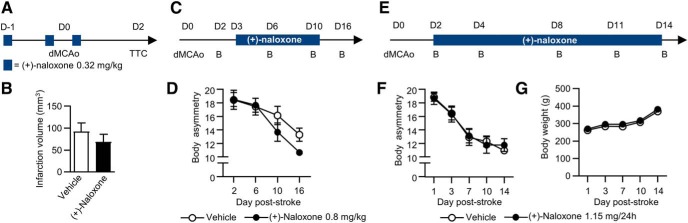
Ischemic stroke is the leading cause of disability, and effective therapeutic strategies are needed to promote complete recovery. Neuroinflammation plays a significant role in stroke pathophysiology, and there is limited understanding of how it affects recovery. The aim of this study was to characterize the spatiotemporal expression profile of microglial activation and whether dampening microglial/macrophage activation post-stroke facilitates the recovery. For dampening microglial/macrophage activation, we chose intranasal administration of naloxone, a drug that is already in clinical use for opioid overdose and is known to decrease microglia/macrophage activation. We characterized the temporal progression of microglia/macrophage activation following cortical ischemic injury in rat and found the peak activation in cortex 7 d post-stroke. Unexpectedly, there was a chronic expression of phagocytic cells in the thalamus associated with neuronal loss. (+)-Naloxone, an enantiomer that reduces microglial activation without antagonizing opioid receptors, was administered intranasally starting 1 d post-stroke and continuing for 7 d. (+)-Naloxone treatment decreased microglia/macrophage activation in the striatum and thalamus, promoted behavioral recovery during the 14-d monitoring period, and reduced neuronal death in the lesioned cortex and ipsilateral thalamus. Our results are the first to show that post-stroke intranasal (+)-naloxone administration promotes short-term functional recovery and reduces microglia/macrophage activation. Therefore, (+)-naloxone is a promising drug for the treatment of ischemic stroke, and further studies should be conducted.
Keywords: Microglia; NF-κB; middle cerebral artery occlusion; naloxone; secondary injury; stroke.
Figures
References
-
- Airavaara M, Chiocco MJ, Howard DB, Zuchowski KL, Peränen J, Liu C, Fang S, Hoffer BJ, Wang Y, Harvey BK (2010) Widespread cortical expression of MANF by AAV serotype 7: localization and protection against ischemic brain injury. Exp Neurol 225:104–113. 10.1016/j.expneurol.2010.05.020 - DOI - PMC - PubMed
-
- Atkinson RL (1984) Endocrine and metabolic effects of opiate antagonists. J Clin Psychiatry 45:20–24. - PubMed
-
- Baskin DS, Hosobuchi Y (1981) Naloxone reversal of ischaemic neurological deficits in man. Lancet 2:272–275. - PubMed
-
- Bederson JB, Pitts LH, Tsuji M, Nishimura MC, Davis RL, Bartkowski H (1986) Rat middle cerebral artery occlusion: evaluation of the model and development of a neurologic examination. Stroke 17:472–476. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical