

Consensus statement on the definition of neurogenic supine hypertension in cardiovascular autonomic failure by the American Autonomic Society (AAS) and the European Federation of Autonomic Societies (EFAS) : Endorsed by the European Academy of Neurology (EAN) and the European Society of Hypertension (ESH)
- PMID: 29766366
- PMCID: PMC6097730
- DOI: 10.1007/s10286-018-0529-8
Consensus statement on the definition of neurogenic supine hypertension in cardiovascular autonomic failure by the American Autonomic Society (AAS) and the European Federation of Autonomic Societies (EFAS) : Endorsed by the European Academy of Neurology (EAN) and the European Society of Hypertension (ESH)
Abstract
Purpose: Patients suffering from cardiovascular autonomic failure often develop neurogenic supine hypertension (nSH), i.e., high blood pressure (BP) in the supine position, which falls in the upright position owing to impaired autonomic regulation. A committee was formed to reach consensus among experts on the definition and diagnosis of nSH in the context of cardiovascular autonomic failure.
Methods: As a first and preparatory step, a systematic search of PubMed-indexed literature on nSH up to January 2017 was performed. Available evidence derived from this search was discussed in a consensus expert round table meeting in Innsbruck on February 16, 2017. Statements originating from this meeting were further discussed by representatives of the American Autonomic Society and the European Federation of Autonomic Societies and are summarized in the document presented here. The final version received the endorsement of the European Academy of Neurology and the European Society of Hypertension.
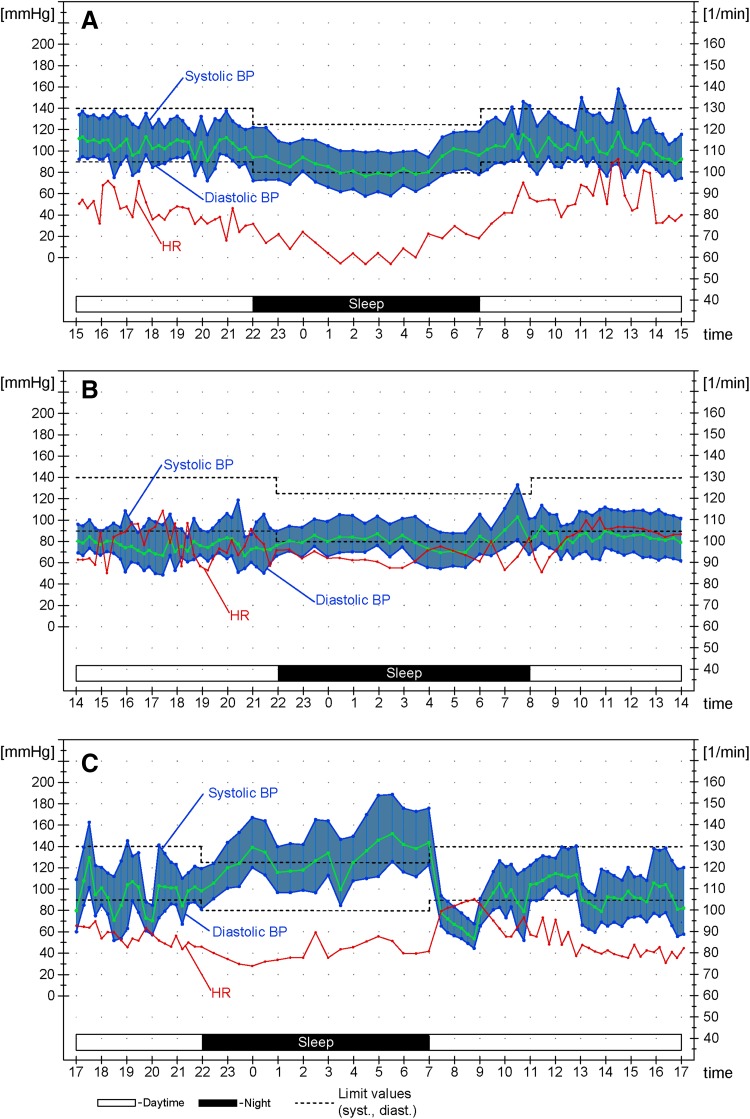
Results: In patients with neurogenic orthostatic hypotension, nSH is defined as systolic BP ≥ 140 mmHg and/or diastolic BP ≥ 90 mmHg, measured after at least 5 min of rest in the supine position. Three severity degrees are recommended: mild, moderate and severe. nSH may also be present during nocturnal sleep, with reduced-dipping, non-dipping or rising nocturnal BP profiles with respect to mean daytime BP values. Home BP monitoring and 24-h-ambulatory BP monitoring provide relevant information for a customized clinical management.
Conclusions: The establishment of expert-based criteria to define nSH should standardize diagnosis and allow a better understanding of its epidemiology, prognosis and, ultimately, treatment.
Keywords: ABPM; Autonomic failure; Neurogenic orthostatic hypotension; Neurogenic supine hypertension; Nocturnal hypertension.
Conflict of interest statement
Alessandra Fanciulli: nothing to declare. Jens Jordan: served as advisor for Janssen-Cilag, Novartis, Novo-Nordisk and Theravance and received research support from Boston Scientific outside of the submitted work; he is also co-founder of Eternygen GmbH. Italo Biaggioni: receives support from the NIH Rare Disease Clinical Research Network (U54-NS065736), reports consultancies for Lundbeck and Theravance for development of drugs to treat orthostatic hypotension and owns a patent application for an automated inflatable binder for the treatment of orthostatic hypotension. Giovanna Calandra–Buonaura: nothing to declare. William P. Cheshire: nothing to declare. Pietro Cortelli: nothing to declare. Sabine Eschlboeck: nothing to declare. Guido Grassi: nothing to declare. Max J. Hilz: nothing to declare. Horacio Kaufmann: receives support from the NIH Rare Disease Clinical Research Network (U54-NS065736). Heinz Lahrmann: nothing to declare. Giuseppe Mancia: nothing to declare. Gert Mayer: nothing to declare. Lucy Norcliffe–Kaufmann: receives support from the NIH Rare Disease Clinical Research Network (U54-NS065736). Anne Pavy-Le Traon: nothing to declare. Satish R. Raj: receives research support from the Canadian Institutes of Health Research (CIHR; Ottawa, ON, Canada) grant MOP142426 and the Cardiac Arrhythmia Network of Canada (CANet; London, ON, Canada) grants SRG-15-P01-001 and SRG-17-P27-001, and the Vanderbilt Institute for Clinical and Translational Research funded by a Clinical and Translational Science Award from the National Center for Advancing Translational Science from the National Institutes of Health (UL1 TR000445); he also reports consultancies for Lundbeck LLC and GE Healthcare. David Robertson: nothing to declare. Isabel Rocha: nothing to declare. Walter Struhal: nothing to declare. Roland Thijs: receives research support from the Dutch National Epilepsy Fund, ZonMW, NUTS Ohra Fund, Medtronic and AC Thomson Foundation, and has received fees for lectures from Medtronic, UCB and GSK. Konstantinos P. Tsioufis: nothing to declare. J. Gert Van Dijk: nothing to declare. Gregor K. Wenning: nothing to declare.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
