

Subclinical inflammation phenotypes and long-term outcomes after pediatric kidney transplantation
- PMID: 29766640
- PMCID: PMC6436389
- DOI: 10.1111/ajt.14933
Subclinical inflammation phenotypes and long-term outcomes after pediatric kidney transplantation
Abstract
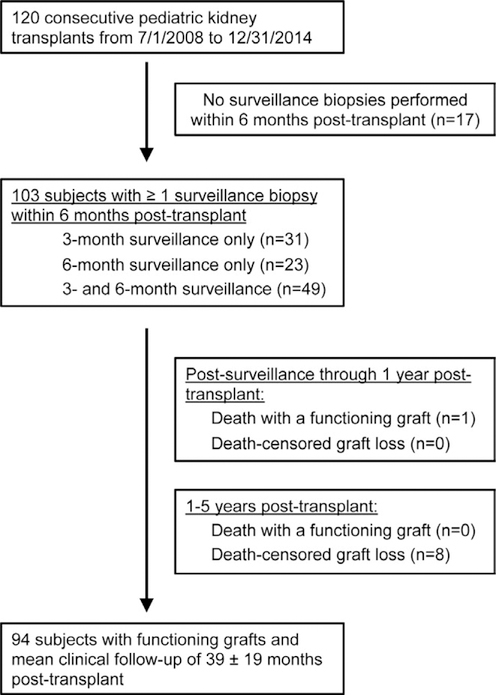
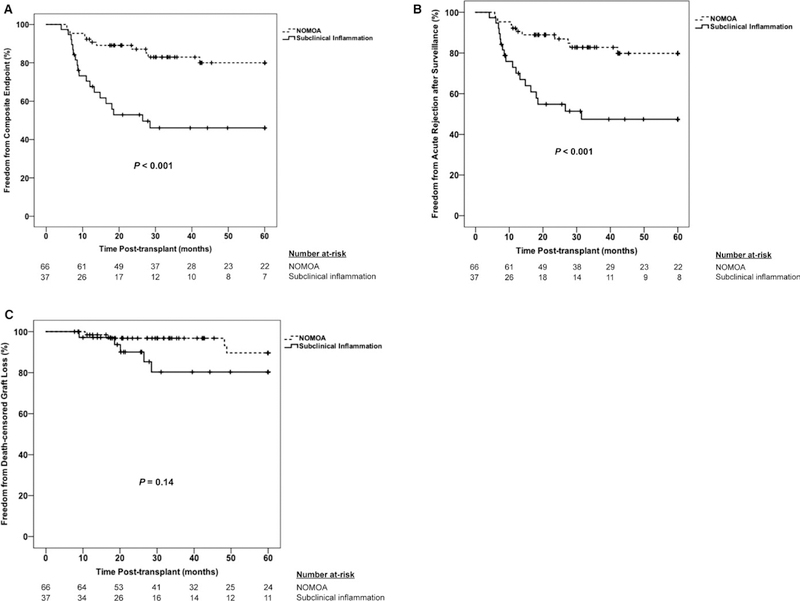
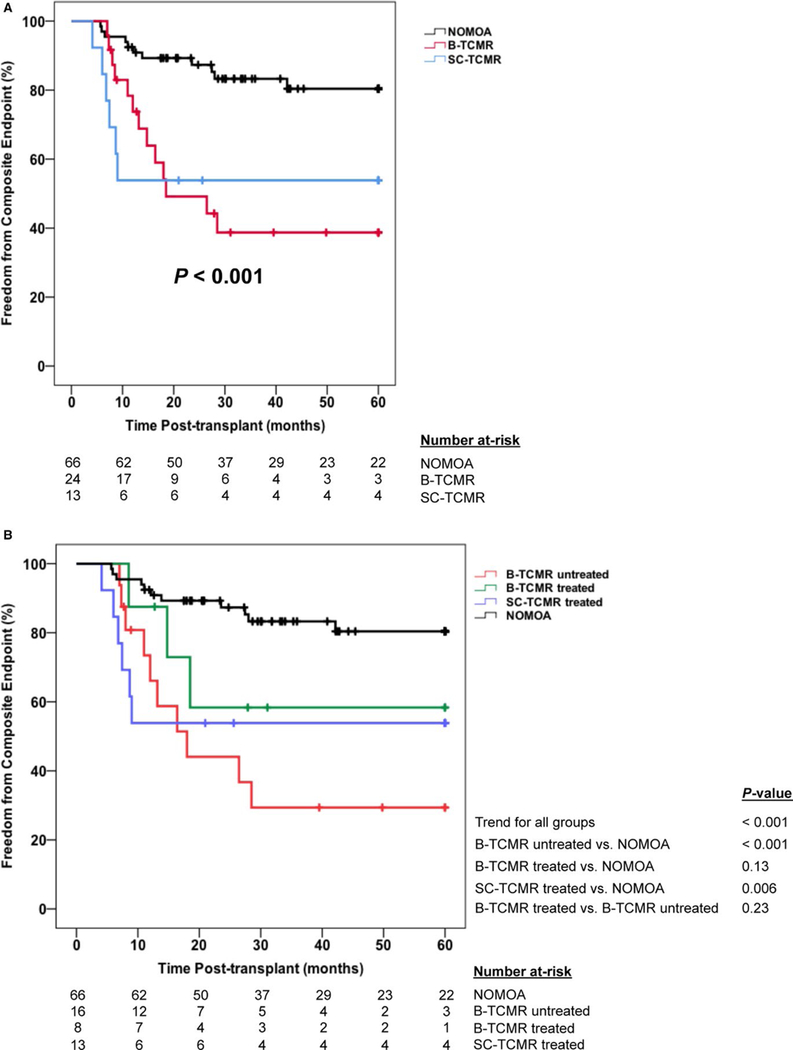
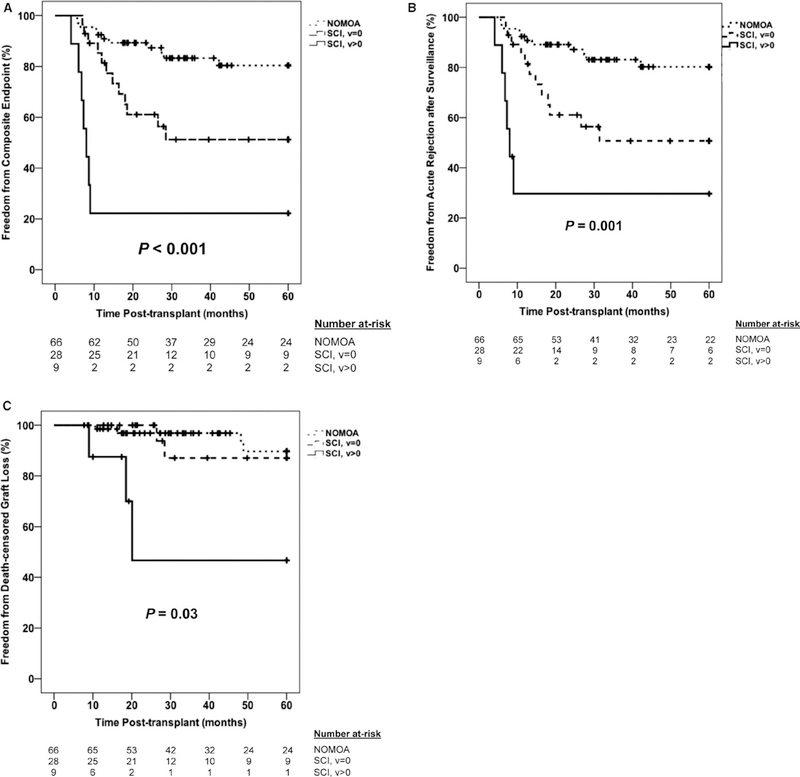
The implementation of surveillance biopsies in pediatric kidney transplantation remains controversial. Surveillance biopsies detect subclinical injury prior to clinical dysfunction, which could allow for early interventions that prolong allograft survival. We conducted a single-center retrospective cohort study of 120 consecutive pediatric kidney recipients, of whom 103 had surveillance biopsies ≤6 months posttransplant. We tested the hypothesis that subclinical inflammation (borderline or T cell-mediated rejection without clinical dysfunction) is associated with a 5-year composite endpoint of acute rejection and allograft failure. Overall, 36% of subjects had subclinical inflammation, which was associated with increased hazard for the composite endpoint (adjusted hazard ratio 2.89 [1.27, 6.57]; P < .01). Subjects with treated vs untreated subclinical borderline rejection had a lower incidence of the composite endpoint (41% vs 67%; P < .001). Subclinical vascular injury (subclinical inflammation with Banff arteritis score > 0) had a 78% incidence of the composite endpoint vs 11% in subjects with no major surveillance abnormalities (P < .001). In summary, we showed that subclinical inflammation phenotypes were prevalent in pediatric kidney recipients without clinical dysfunction and were associated with increased acute rejection and allograft failure. Once prospectively validated, our data would support implementation of surveillance biopsies as standard of care in pediatric kidney transplantation.
Keywords: biopsy; clinical research/practice; graft survival; kidney transplantation/nephrology; pathology/histopathology; pediatrics; protocol biopsy; rejection: subclinical; rejection: vascular.
© 2018 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
DISCLOSURE
The authors of this manuscript have no conflicts of interest to disclose as described by the
Figures
References
-
- Lodhi SA, Lamb KE, Meier-Kriesche HU. Solid organ allograft survival improvement in the United States: the long-term does not mirror the dramatic short-term success. Am J Transplant 2011;11(6):1226–1235. - PubMed
-
- Meier-Kriesche HU, Schold JD, Srinivas TR, Kaplan B. Lack of improvement in renal allograft survival despite a marked decrease in acute rejection rates over the most recent era. Am J Transplant 2004;4(3):378–383. - PubMed
-
- El-Zoghby ZM, Stegall MD, Lager DJ, et al. Identifying specific causes of kidney allograft loss. Am J Transplant 2009;9(3):527–535. - PubMed
-
- Famulski KS, Reeve J, de Freitas DG, Kreepala C, Chang J, Halloran PF. Kidney transplants with progressing chronic diseases express high levels of acute kidney injury transcripts. Am J Transplant 2013;13(3):634–644. - PubMed
-
- Walsh RC, Brailey P, Girnita A, et al. Early and late acute antibody-mediated rejection differ immunologically and in response to proteasome inhibition. Transplantation 2011;91(11):1218–1226. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
