

Impact of new DAA therapy on real clinical practice: a multicenter region-wide cohort study
- PMID: 29769038
- PMCID: PMC5956792
- DOI: 10.1186/s12879-018-3125-6
Impact of new DAA therapy on real clinical practice: a multicenter region-wide cohort study
Abstract
Background: Management of chronic hepatitis C (CHC) has significantly accelerated in the last few years. Currently, second generation direct acting antivirals (DAAs) promise clearance of infection in most of patients. Here we present the results of the first analysis carried out on data of Lazio clinical network for DAAs.
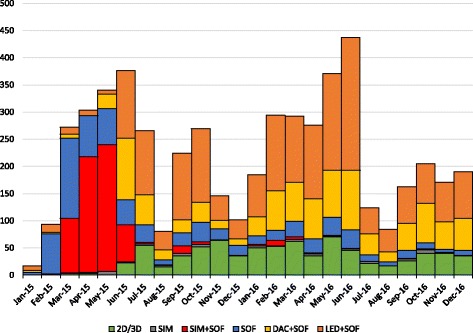
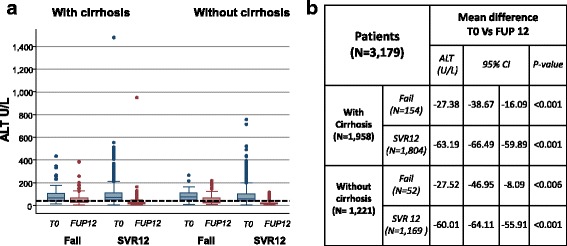
Methods: The study was designed as a multicenter cohort: a) to assess the evolution of treatment during the first 24 months of the activity of the Clinical Network; b) to report overall efficacy of treatments; c) to analyze potential factors associated with lack of virological response at 12 weeks after therapy (SVR12); d) to evaluate the variation of ALT at baseline and 12 weeks after therapy in those who achieved SVR12 in comparison to those who did not. Analyses of efficacy were carried out with multilevel mixed effect logistic regression model. ALT temporal variation was assessed by mixed effect model mixed models with random intercept at patient's level and random slope at the level of the time; i.e. either before or after therapy.
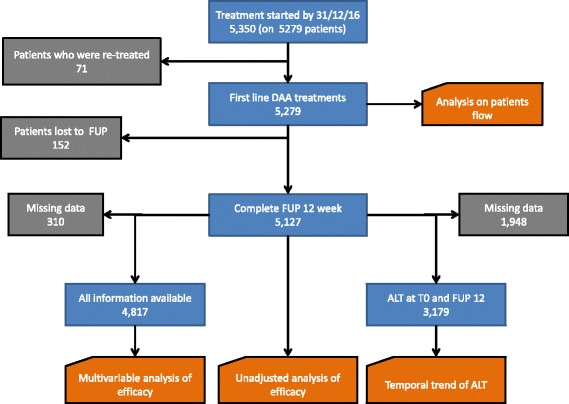
Results: Between 30 December 2014 and 31 December 2016 5279 patients started a DAA treatment; of those, 5127 (in 14 clinical centers) had completed the 12-week follow-up. Overall proportion of SVR12 was 93.41% (N = 4780) with no heterogeneity between the 14 clinical centers. Interruption as the consequence of severe side effect was very low (only 23 patients). Unadjusted analysis indicates that proportion of SVR12 significantly changes according to patient's baseline characteristics, however after adjusting for potential confounders only adherence to current guidelines, stage of liver diseases, gender, transplant and HIV status were independently associated with the response to therapy. Analysis of ALT temporal variation showed that ALT level normalized in most, but not, all patients who achieved SVR12.
Conclusion: Our study confirmed the extraordinary efficacy of DAAs outside clinical trials. The advantage of DAAs was particularly significant for those patients who were previously considered as difficult-to-treat and did not have treatment options before DAAs era. Intervention based on network of select centers and prioritization of patients according to diseases severity was successful. Further studies are needed to establish whether clearance of HCV after DAAs therapy can arrest or even revert liver fibrosis in non-cirrhotic patients and/or improve life quality and expectancy in those who achieve SVR12 with cirrhosis.
Keywords: Chronic hepatitis C; Clinical study; Direct acting antiviral; Hepatitis C virus; Liver cirrhosis; Liver damage; Mixed effect model; Multicenter cohort study; New therapy; Treatment efficacy.
Conflict of interest statement
Ethics approval and consent to participate
This study was carried out within the institutional mandate of the Lazio Region Health Authority to the Lazio Regional Service for Epidemiology and Surveillance of Infectious Diseases (SeRESMI). The terms of SeRESMI mandate and utilization of data collected are established by a Regional law and includes monitoring access to therapy with DAA, monitoring therapy outcome and implementation of periodical analyses for administrative and scientific purposes. Patients signed informed consent for use of anonymous information accordingly with the Regional act which has enforced the clinical network. Patients’ data were collected through an on-line system and only physicians who have patients in care had access to patients’ personal information. Patients received treatment according to clinical judgment, current availability of drugs and current guidelines at the time they started therapy. We have received the consent for publishing the information contained in the study by the ethics committee of INMI Lazzaro Spallanzani.
Competing interests
CFP has received research grants, lecturing fees, advisory boards, scientific consultancies for Abbvie, Gilead Sciences, BMS, Janssen Cilag, VIIV, Roche, Abbott Diagnostics. EG has received personal fees from Gilead Sciences, Janssen, Otsuka Novel Products and Angelini for consultancy or lectures, outside the submitted work. GDO has received personal fees for Speaking, teaching and participation to advisory board for: Gilead, BMS, MSD. MA: has received grants for fellowship, research and participation to international meetings form Abbvie, Gilead, Janssen, MSD, he participated to advisory board for Gilead and Abbvie. GT: has received Traveling and speaking fees from Abbvie, BMS, Gilead, MSD. AP: has received grants for participation to meeting form: MSD, Gilead, Bristol Meyer Squibb. ADS: has received traveling and speaking fees from Abbvie and Gilead. AG: has received grants for fellowship, research and participation to international meetings form Abbvie, Gilead, Janssen, Alfa Wassermann, CD INV, Sigma Tau, Takeda, MSD; he participated to advisory board for Gilead, CD INV, Sigma Tau, Alfa Wassermann and Abbvie. FSM has received grants for fellowship, research and participation to international meetings form Abbvie, Gilead, Janssen, MSD; he participated to advisory board for Abbvie, Gilead, Janssen and MSD. GI, SL, VP, PS VV, MS, AM, LL, FC, OA, AFA, declare no competing interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- WHO. Hepatitis C Fact sheet N°164. http://www.who.int/en/news-room/fact-sheets/detail/hepatitis-c. Accessed 05 May 2018.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
