

Predictors of Length of Hospital Stay After Complete Repair for Tetralogy of Fallot: A Prospective Cohort Study
- PMID: 29769202
- PMCID: PMC6015346
- DOI: 10.1161/JAHA.118.008719
Predictors of Length of Hospital Stay After Complete Repair for Tetralogy of Fallot: A Prospective Cohort Study
Abstract
Background: We sought to identify patient and surgical factors associated with time to hospital discharge in patients undergoing complete repair for tetralogy of Fallot.
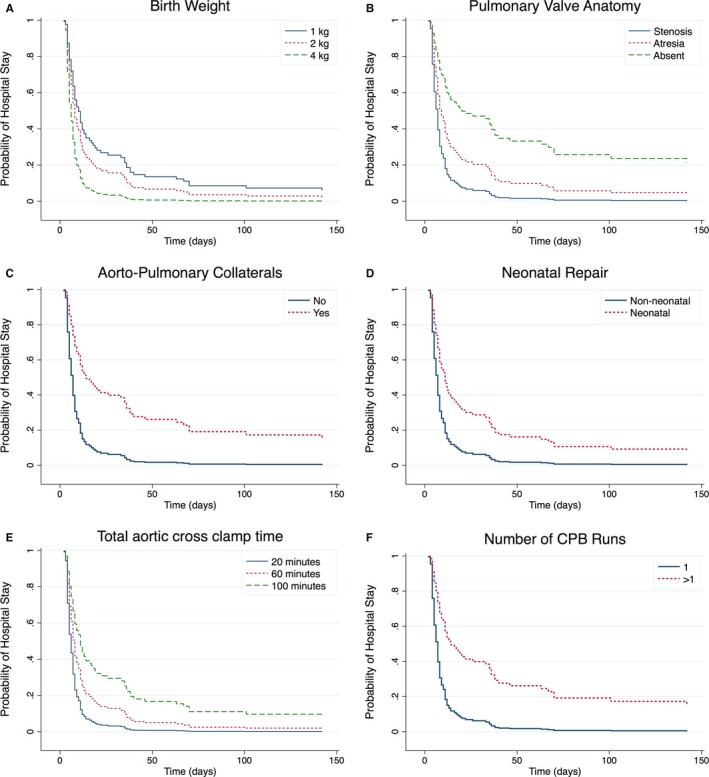
Methods and results: We performed a prospective cohort study of patients with tetralogy of Fallot admitted for complete repair between May 1, 2012 and June 2, 2017 at Children's Hospital of Philadelphia with detailed demographic, clinical, and operative characteristics. The primary outcome was time to hospital discharge. Cox proportional hazards models were used to identify patient and operative predictors of time to hospital discharge. We enrolled 151 subjects, 62.8% male, 65.6% non-Hispanic white, and 9.9% non-Hispanic black. The median time to hospital discharge was 7 days (interquartile range 4, 12). Five patients died in the hospital, all of whom underwent tetralogy of Fallot repair beyond the neonatal period. Greater birth weight was associated with higher rate of hospital discharge (hazard ratio [HR]=1.35, 95% confidence interval (CI) =1.11, 1.64), while absent pulmonary valve versus pulmonary stenosis (HR=0.27, 95% CI=0.08, 0.91), pulmonary valve atresia versus pulmonary stenosis (HR=0.57, 95% CI=0.33, 0.97), presence of aortopulmonary collaterals (HR=0.44, 95% CI=0.24, 0.84), complete repair performed in the neonatal period (<30 days of life) (HR=0.45, 95% CI=0.27, 0.75), more than 1 cardiopulmonary bypass run (HR=0.33, 95% CI=0.18, 0.61), and longer aortic cross-clamp time (HR [per 10 minutes]=0.88, 95% CI=0.79, 0.97) were associated with lower rate of hospital discharge.
Conclusions: Postoperative hospital stay after complete repair of tetralogy of Fallot is in part determined by patient and operative factors. Some (eg, surgical strategy for the symptomatic neonate) may be modifiable. These results may impact patient counseling, choice of surgical approach, and postoperative care.
Keywords: hospital stay; outcome; surgery; tetralogy of Fallot.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Liu M, Druschel CM, Hannan EL. Risk‐adjusted prolonged length of stay as an alternative outcome measure for pediatric congenital cardiac surgery. Ann Thorac Surg. 2014;97:2154–2159. - PubMed
-
- Welke KF, Karamlou T, Ungerleider RM, Diggs BS. Mortality rate is not a valid indicator of quality differences between pediatric cardiac surgical programs. Ann Thorac Surg. 2010;89:139–144; discussion 145‐146. - PubMed
-
- Jacobs JP, Jacobs ML, Austin EH III, Mavroudis C, Pasquali SK, Lacour‐Gayet FG, Tchervenkov CI, Walters H III, Bacha EA, Nido PJ, Fraser CD, Gaynor JW, Hirsch JC, Morales DL, Pourmoghadam KK, Tweddell JS, Prager RL, Mayer JE. Quality measures for congenital and pediatric cardiac surgery. World J Pediatr Congenit Heart Surg. 2012;3:32–47. - PMC - PubMed
-
- Limperopoulos C, Majnemer A, Shevell MI, Rohlicek C, Rosenblatt B, Tchervenkov C, Darwish HZ. Predictors of developmental disabilities after open heart surgery in young children with congenital heart defects. J Pediatr. 2002;141:51–58. - PubMed
-
- Newburger JW, Wypij D, Bellinger DC, du Plessis AJ, Kuban KC, Rappaport LA, Almirall D, Wessel DL, Jonas RA, Wernovsky G. Length of stay after infant heart surgery is related to cognitive outcome at age 8 years. J Pediatr. 2003;143:67–73. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
