

Early and Chronic Dipeptidyl-Peptidase-IV Inhibition and Cardiovascular Events in Patients With Type 2 Diabetes Mellitus After an Acute Coronary Syndrome: A Landmark Analysis of the EXAMINE Trial
- PMID: 29769203
- PMCID: PMC6015373
- DOI: 10.1161/JAHA.117.007649
Early and Chronic Dipeptidyl-Peptidase-IV Inhibition and Cardiovascular Events in Patients With Type 2 Diabetes Mellitus After an Acute Coronary Syndrome: A Landmark Analysis of the EXAMINE Trial
Abstract
Background: Antihyperglycemic therapies may increase the risk of cardiovascular events including hospitalization for heart failure. There is a paucity of data evaluating the cardiovascular safety of antihyperglycemic therapies in the high-risk period following an acute coronary syndrome (ACS).
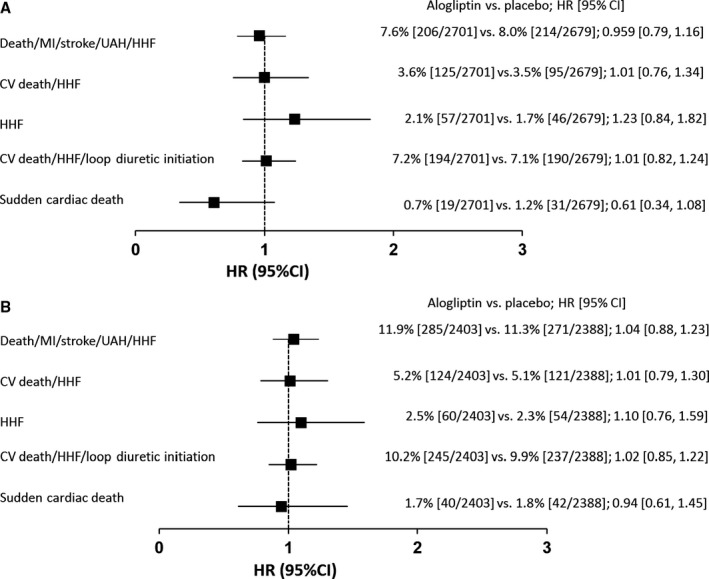
Methods and results: The EXAMINE (Examination of Cardiovascular Outcomes with Alogliptin versus Standard of Care) trial randomized 5380 patients who were 15 to 90 days post ACS to the dipeptidyl dipeptidase-IV (DPP-IV) inhibitor alogliptin versus placebo; mean follow-up was 18 months. Using a landmark analysis, we assessed the (1) burden of cardiovascular events from randomization to 6 months (early period) and from 6 months to the end of follow-up (late period) and (2) the risk of cardiovascular events associated with early (up to 6 months) and chronic (6 months to end of follow-up) DPP-IV inhibition with alogliptin. Patients with early versus late events had similar baseline demographic profiles. Overall, 42.1% of the composite of cardiovascular death/myocardial infarction/stroke and 47.5% of hospitalization for heart failure occurred in the early period. Early DPP-IV inhibition did not increase the risk of early cardiovascular death/myocardial infarction/stroke (hazard ratio 0.96, 95% confidence interval, 0.76-1.21) or hospitalization for heart failure (1.23, 95% confidence interval, 0.84-1.82). Similarly, chronic DPP-IV inhibition did not increase the risk of late cardiovascular death/myocardial infarction/stroke (hazard ratio 1.03, 95% confidence interval, 0.89-1.26) or hospitalization for heart failure (hazard ratio 1.02, 95% confidence interval, 0.85-1.22).
Conclusions: Early after an ACS, patients with type 2 diabetes mellitus experience a significant burden of HF events and recurrent ACS. DPP-IV inhibition with alogliptin appears to be safe even in the high-risk period following an ACS.
Trial registration: ClinicalTrials.gov NCT00968708.
Keywords: acute coronary syndrome; alogliptin; diabetes mellitus; dipeptidyl dipeptidase‐4 inhibitor; medical therapy; medication.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures




References
-
- American Diabetes Association . Standards of medical care in diabetes 2016. Cardiovascular disease and risk management. Diabetes Care. 2016;39(suppl 1):S60–S71. - PubMed
-
- Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, Peters AL, Tsapas A, Wender R, Matthews DR. Management of hyperglycaemia in type 2 diabetes, 2015: a patient‐centred approach. Update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia. 2015;58:429–442. - PubMed
-
- Swedberg K, Rydén L. Treatment of diabetes and heart failure: joint forces. Eur Heart J. 2016;37:1535–1537. - PubMed
-
- Dei Cas A, Khan SS, Butler J, Khan SS, Butler J, Mentz RJ, Bonow RO, Avogaro A, Tschoepe D, Doehner W, Greene SJ, Senni M, Gheorghiase M, Fonarow GC. Impact of diabetes on epidemiology, treatment, and outcomes of patients with heart failure. JACC Heart Fail. 2015;3:136–145. - PubMed
-
- Sharma A, Ezekowitz JA. Diabetes, impaired fasting glucose, and heart failure: its not all about the sugar. Eur J Heart Fail. 2014;16:1153–1156. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
