

Pulmonary function tests as outcomes for systemic sclerosis interstitial lung disease
- PMID: 29769294
- PMCID: PMC9488607
- DOI: 10.1183/16000617.0102-2017
Pulmonary function tests as outcomes for systemic sclerosis interstitial lung disease
Abstract
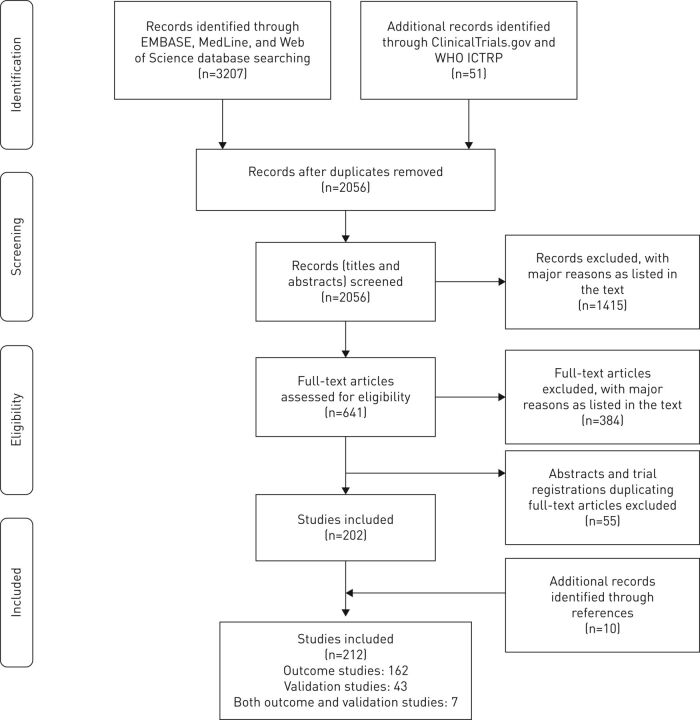
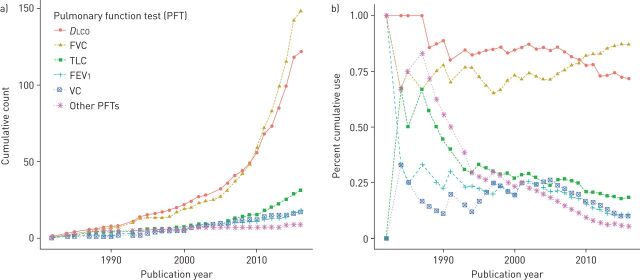
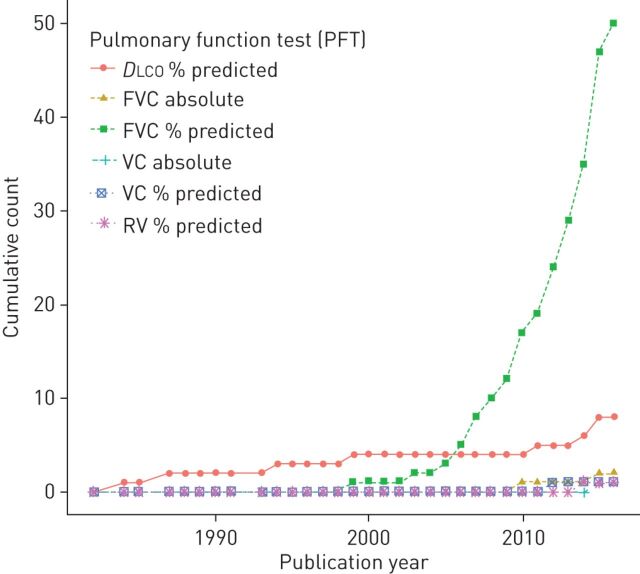
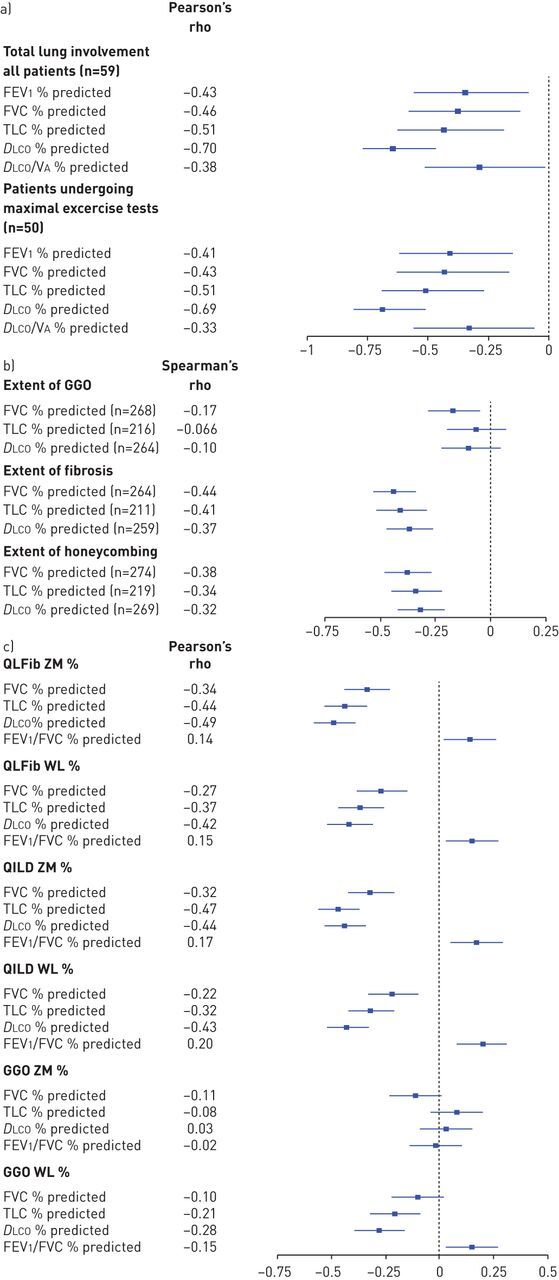
Interstitial lung disease (ILD) is the leading cause of morbidity and mortality in systemic sclerosis (SSc). We performed a systematic review to characterise the use and validation of pulmonary function tests (PFTs) as surrogate markers for systemic sclerosis-associated interstitial lung disease (SSc-ILD) progression.Five electronic databases were searched to identify all relevant studies. Included studies either used at least one PFT measure as a longitudinal outcome for SSc-ILD progression (i.e. outcome studies) and/or reported at least one classical measure of validity for the PFTs in SSc-ILD (i.e. validation studies).This systematic review included 169 outcome studies and 50 validation studies. Diffusing capacity of the lung for carbon monoxide (DLCO) was cumulatively the most commonly used outcome until 2010 when it was surpassed by forced vital capacity (FVC). FVC (% predicted) was the primary endpoint in 70.4% of studies, compared to 11.3% for % predicted DLCO Only five studies specifically aimed to validate the PFTs: two concluded that DLCO was the best measure of SSc-ILD extent, while the others did not favour any PFT. These studies also showed respectable validity measures for total lung capacity (TLC).Despite the current preference for FVC, available evidence suggests that DLCO and TLC should not yet be discounted as potential surrogate markers for SSc-ILD progression.
Copyright ©ERS 2018.
Conflict of interest statement
Conflict of interest: M. Caron reports grants from the Fonds de Recherche du Québec (Santé PhD Studentship) and from the Canadian Institutes of Health Research (GSD–146268) during the conduct of the study. S. Hoa reports grants from the Université de Montréal Rheumatology Clinical Fellowship Program (Abbvie educational grant) and from the Arthritis Society's Postdoctoral Fellowship Award, during the conduct of the study.
Figures
References
-
- Gabrielli A, Avvedimento EV, Krieg T. Scleroderma. N Engl J Med 2009; 360: 1989–2003. - PubMed
-
- Katsumoto TR, Whitfield ML, Connolly MK. The pathogenesis of systemic sclerosis. Annu Rev Pathol 2011; 6: 509–537. - PubMed
-
- Seibold J. Scleroderma. In: Harris ED, Budd RC, Firestein GS, Genovese MC, Sergent JS, Ruddy S, Sledge CB, eds. Kelley's Textbook of Rheumatology. 7th Edn. Philadelphia, Elsevier, 2005; pp. 1279–1308.
-
- Steele R, Hudson M, Lo E, et al. . Clinical decision rule to predict the presence of interstitial lung disease in systemic sclerosis. Arthritis Care Res (Hoboken) 2012; 64: 519–524. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical