

Acute Glaucoma Attack Following Microvascular Decompression Surgery for Trigeminal Neuralgia
- PMID: 29769452
- PMCID: PMC6002677
- DOI: 10.2176/nmc.cr.2017-0251
Acute Glaucoma Attack Following Microvascular Decompression Surgery for Trigeminal Neuralgia
Abstract
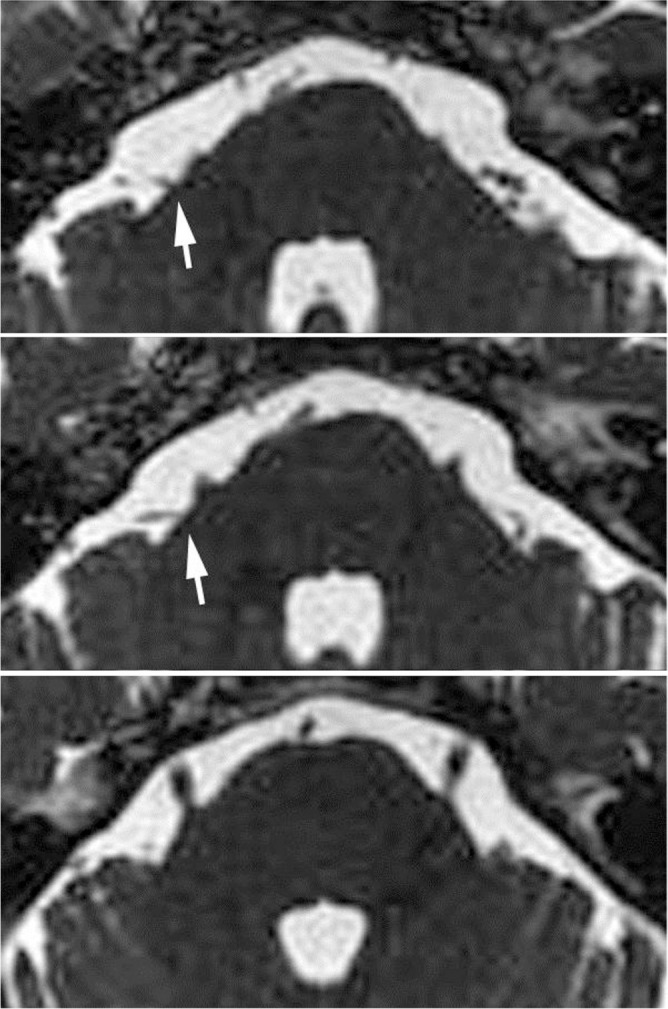
Microvascular decompression (MVD) is widely accepted as an effective surgical method to treat trigeminal neuralgia (TN), but the risks of morbidity and mortality must be considered. We experienced a case of acute angle-closure glaucoma attack following MVD for TN in an elderly patient, considered to be caused by lateral positioning during and after the surgery. A 79-year-old female underwent MVD for right TN in the left lateral decubitus position, and TN disappeared after the surgery. Postoperatively, the patient tended to maintain the left lateral decubitus position to prevent wound contact with the pillow, even after ambulation. Two days after the surgery, she complained of persistent left ocular pain with visual disturbance. The left pupil was dilated with only light perception, and the intraocular pressure (IOP) was 44 mmHg. Acute angle-closure glaucoma attack was diagnosed. After drip infusion of mannitol, emergent laser iridotomy was performed. The corrected visual acuity recovered with normalization of IOP (14 mmHg). The subsequent clinical course was uneventful and she was discharged from our hospital. The left lateral positioning during and after the surgery was considered to have contributed to increase IOP of the eye on the dependent side, which resulted in acute angle-closure glaucoma attack. The potential pathology is difficult to assess preoperatively, but patient management should always consider the increased possibility of this condition with age.
Keywords: complication; glaucoma; lateral decubitus position; microvascular decompression; trigeminal neuralgia.
Conflict of interest statement
The authors report on conflict of interest concerning the materials or methods used in this study or findings specific to the article. All authors who are members of The Japan Neurosurgery Society (JNS) have registered online self-reported COI disclosure statement forms through the website for JNS members.
Figures



References
-
- Barker FG, Jannetta PJ, Bissonette DJ, Larkins MV, Jho HD: The long-term outcome of microvascular decompression for trigeminal neuralgia. N Engl J Med 334: 1077– 1083, 1996. - PubMed
-
- Hanakita J, Kondo A: Serious complications of microvascular decompression operations for trigeminal neuralgia and hemifacial spasm. Neurosurgery 22: 348– 352, 1988. - PubMed
-
- Maesawa S, Salame C, Flickinger JC, Pirris S, Kondziolka D, Lunsford LD: Clinical outcomes after stereotactic radiosurgery for idiopathic trigeminal neuralgia. J Neurosurg 94: 14– 20, 2001. - PubMed
-
- Kouzounias K, Lind G, Schechtmann G, Winter J, Linderoth B: Comparison of percutaneous balloon compression and glycerol rhizotomy for the treatment of trigeminal neuralgia. J Neurosurg 113: 486– 492, 2010. - PubMed
-
- Kanpolat Y, Savas A, Bekar A, Berk C: Percutaneous controlled radiofrequency trigeminal rhizotomy for the treatment of idiopathic trigeminal neuralgia: 25-year experience with 1,600 patients. Neurosurgery 48: 524– 534, 2001. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical