Evaluation of periosteum eversion and coronally advanced flap techniques in the treatment of isolated Miller's Class I/II gingival recession: A comparative clinical study
- PMID: 29769769
- PMCID: PMC5939022
- DOI: 10.4103/jisp.jisp_5_18
Evaluation of periosteum eversion and coronally advanced flap techniques in the treatment of isolated Miller's Class I/II gingival recession: A comparative clinical study
Abstract
Aim: The present investigation aimed to evaluate root coverage (RC) with periosteum eversion technique (PET) using periosteum as a graft and coronally advanced flap (CAF) with platelet-rich fibrin (PRF) membrane as a graft in the treatment of isolated Miller's class I and II gingival recession defects.
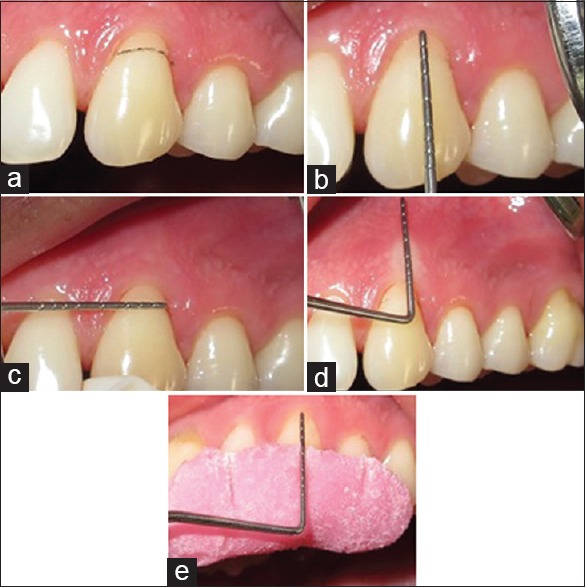
Materials and methods: Thirty sites in 15 participants with Miller's Class I or II gingival recession were randomly treated either with PET using periosteum as graft and CAF + PRF as graft. In a split mouth design, the parameters such as recession depth, recession width at cementoenamel junction, probing depth, periodontal attachment level (PAL), and keratinized gingival width were assessed at baseline, 3 months, and 6 months postoperative follow-up with William's graduated probe and Vernier caliper.
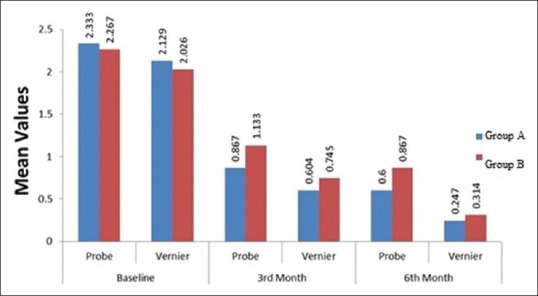
Results: Both the treatment modalities yielded statistically nonsignificant desirable treatment outcomes at both postoperative levels in terms of all the parameters The mean RC with probe method and Vernier method in CAF + PRF was 75.01% and 86.86%, respectively, and PET showed a mean RC of 61.112% and 83.971%, respectively, at 6-month interval period which showed a nonstatistically significant difference.
Conclusion: Both the treatment modalities, i.e., CAF + PRF and PET are essentially and equally effective in the treatment of Miller's Class I or II gingival recession defects.
Keywords: Coronally advanced flap; periosteum eversion technique; platelet-rich fibrin; root coverage.
Conflict of interest statement
There are no conflicts of interest.
Figures


















References
-
- Glossary of Periodontal Terms. 4th ed. Chicago: American Academy of Periodontology; 2001. The American Academy of Periodontology; p. 44.
-
- Roccuzzo M, Bunino M, Needleman I, Sanz M. Periodontal plastic surgery for treatment of localized gingival recessions: A systematic review. J Clin Periodontol. 2002;29(Suppl 3):178–94. - PubMed
-
- Lindhe J, Lang N, Karring T. Mucogingival therapy. Periodontal plastic surgery. In: Ermes E, editor. Clinical Periodontology and Implant Dentistry. 6th ed. Oxford: Blackwell Munksgaard; 2008. pp. 995–1043.
-
- Zucchelli G, De Sanctis M. Treatment of multiple recession-type defects in patients with esthetic demands. J Periodontol. 2000;71:1506–14. - PubMed
-
- Melcher AH. On the repair potential of periodontal tissues. J Periodontol. 1976;47:256–60. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical