

Measles surveillance in Canada: Trends for 2013
- PMID: 29769844
- PMCID: PMC5864443
- DOI: 10.14745/ccdr.v40i12a01
Measles surveillance in Canada: Trends for 2013
Abstract
Objective: The objective of this report is to describe measles activity in Canada during 2013, in order to support the documentation and maintenance of measles elimination status.
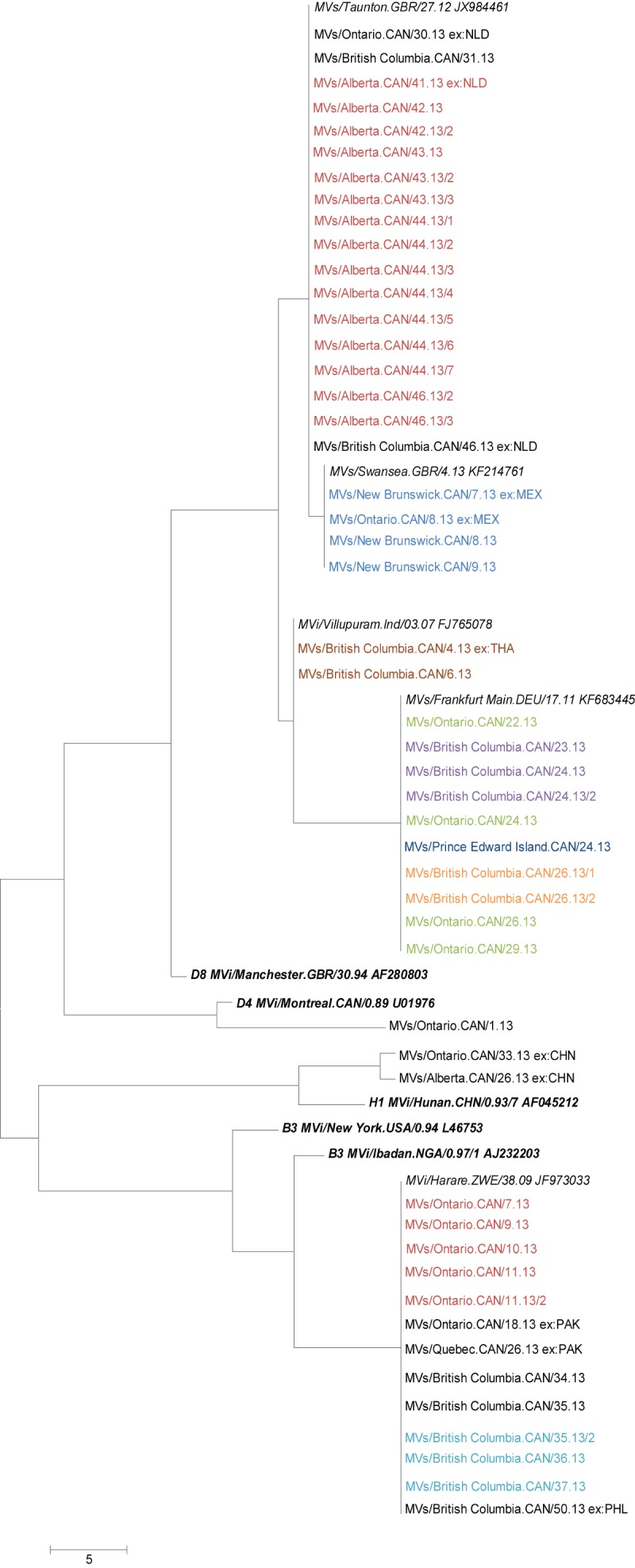
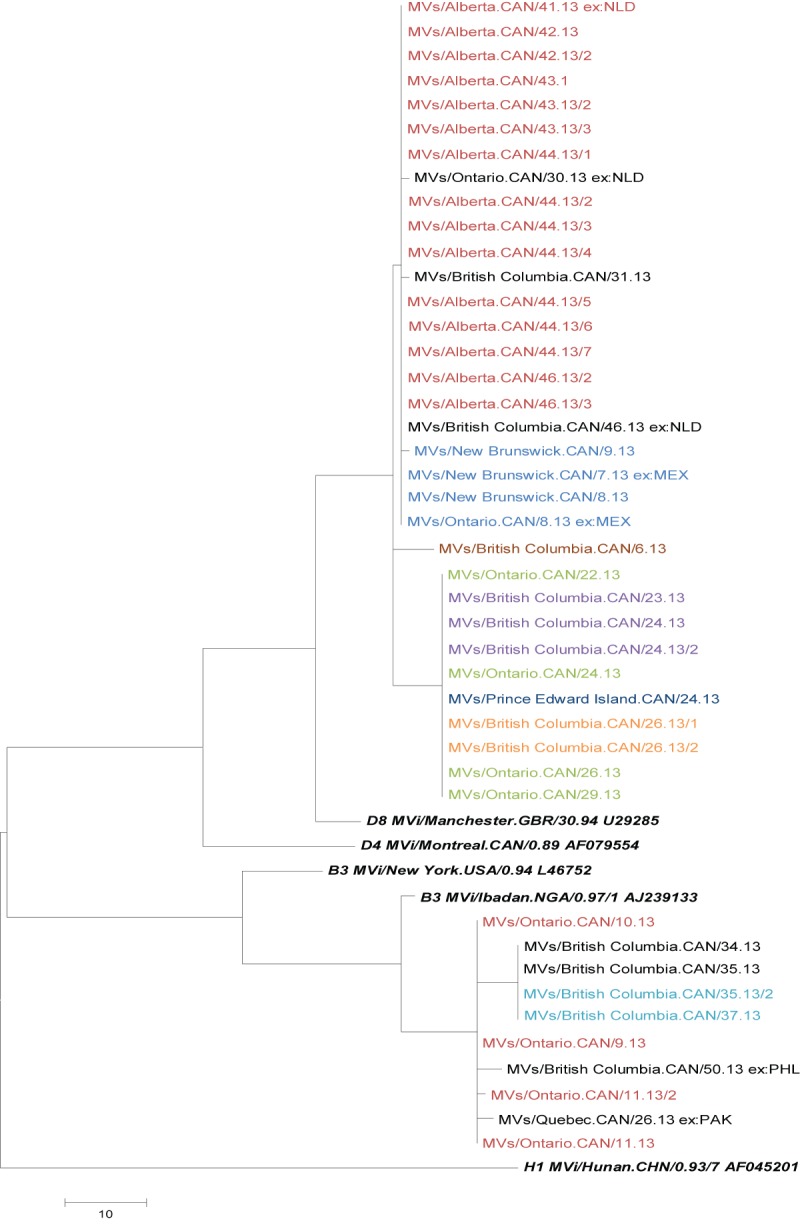
Methods: A descriptive analysis of measles counts and incidence by age group, immunization history, hospitalization and province/territory, as well as a summary of 2013 outbreaks, was conducted using enhanced measles data captured through the Canadian Measles and Rubella Surveillance System. Genotype information and phylogenetic analysis for 2013 were summarized.
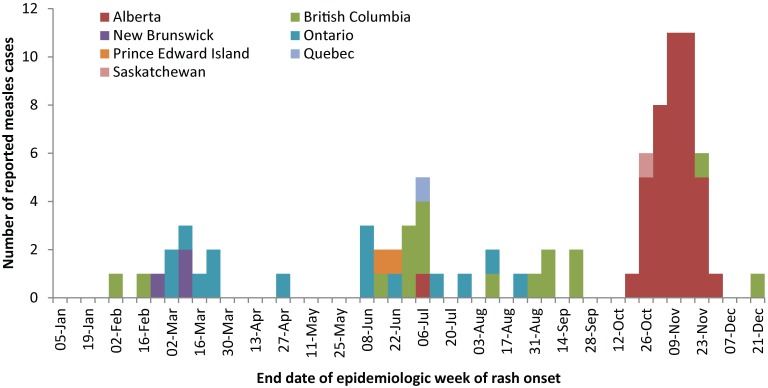
Results: In 2013, 83 confirmed measles cases were reported in seven provinces/territories for an incidence rate of 2.4 per 1,000,000 population. Incidence was highest in the youngest age groups (< 1 year, 1 to 4 years). Burden of disease was highest in the youngest age groups and children 10 to 14 years. Three-quarters of cases had been inadequately immunized, and 10% were hospitalized. There were nine measles outbreaks reported in 2013, one of which consisted of 42 cases in a non-immunizing community in Alberta.
Discussion: 2013 saw the fifth highest number of reported measles cases since 1998. While we continue to face challenges related to importation and heterogeneous immunization coverage, in 2013 Canada met or partially met all four criteria outlined by the Pan American Health Organization for measles elimination.
Conflict of interest statement
Conflicts of interest: There are no conflicts of interest to declare.
Figures
Similar articles
-
Measles surveillance in Canada: 2015.Can Commun Dis Rep. 2016 Jul 7;42(7):139-145. doi: 10.14745/ccdr.v42i07a01. eCollection 2016 Jul 7. Can Commun Dis Rep. 2016. PMID: 29770019 Free PMC article.
-
Measles surveillance in Canada: Trends for 2014.Can Commun Dis Rep. 2015 Jul 2;41(7):157-168. doi: 10.14745/ccdr.v41i07a01. eCollection 2015 Jul 2. Can Commun Dis Rep. 2015. PMID: 29769947 Free PMC article.
-
Measles surveillance in Canada: 2018.Can Commun Dis Rep. 2020 Apr 2;46(4):77-83. doi: 10.14745/ccdr.v46i04a04. eCollection 2020 Apr 2. Can Commun Dis Rep. 2020. PMID: 32558823 Free PMC article.
-
Measles, mumps, rubella prevention: how can we do better?Expert Rev Vaccines. 2021 Jul;20(7):811-826. doi: 10.1080/14760584.2021.1927722. Epub 2021 Jun 7. Expert Rev Vaccines. 2021. PMID: 34096442 Review.
-
Measles and Rubella Global Strategic Plan 2012-2020 midterm review report: Background and summary.Vaccine. 2018 Jan 11;36 Suppl 1:A35-A42. doi: 10.1016/j.vaccine.2017.10.065. Vaccine. 2018. PMID: 29307368 Review.
Cited by
-
Measles surveillance in Canada: 2015.Can Commun Dis Rep. 2016 Jul 7;42(7):139-145. doi: 10.14745/ccdr.v42i07a01. eCollection 2016 Jul 7. Can Commun Dis Rep. 2016. PMID: 29770019 Free PMC article.
-
Applications of geographic information systems in public health: A geospatial approach to analyzing MMR immunization uptake in Alberta.Can J Public Health. 2015 Jun 18;106(6):e355-61. doi: 10.17269/cjph.106.4981. Can J Public Health. 2015. PMID: 26680425 Free PMC article.
-
Measles Outbreak with Unique Virus Genotyping, Ontario, Canada, 2015.Emerg Infect Dis. 2017 Jul;23(7):1063-1069. doi: 10.3201/eid2307.161145. Emerg Infect Dis. 2017. PMID: 28628461 Free PMC article.
-
User-Driven Comments on a Facebook Advertisement Recruiting Canadian Parents in a Study on Immunization: Content Analysis.JMIR Public Health Surveill. 2018 Sep 20;4(3):e10090. doi: 10.2196/10090. JMIR Public Health Surveill. 2018. PMID: 30249585 Free PMC article.
-
The challenges of sustaining measles elimination in Canada.Can Commun Dis Rep. 2014 Jun 12;40(12):261-264. doi: 10.14745/ccdr.v40i12a07. eCollection 2014 Jun 12. Can Commun Dis Rep. 2014. PMID: 29769850 Free PMC article.
References
-
- Pan-American Health Organization (PAHO). Plan of Action: Documentation and verification of measles, rubella and congenital rubella syndrome elimination in the region of the Americas. Technical document. 2010. - PubMed
-
- World Health Organization. Global measles and rubella strategic plan 2012-2020. http://www.refworks.com/refworks2/default.aspx?r=references|MainLayout:init
-
- Public Health Agency of Canada. Elimination of measles, rubella and congenital rubella syndrome in Canada: Documentation and verification report. 2011.
LinkOut - more resources
Full Text Sources
Miscellaneous
