

Enhanced surveillance of invasive meningococcal disease in Canada, 2006-2011
- PMID: 29769898
- PMCID: PMC5864469
- DOI: 10.14745/ccdr.v40i09a01
Enhanced surveillance of invasive meningococcal disease in Canada, 2006-2011
Abstract
Objective: The purpose of this report is to describe the epidemiology of invasive meningococcal disease (IMD) in Canada from 2006 to 2011.
Methods: Data from the Enhanced Invasive Meningococcal Disease Surveillance System and national population estimates were selected for descriptive and inferential analyses. The geographic, demographic, seasonal and subtype distributions as well as clinical characteristics of the IMD cases were examined. Incidence and mortality rates were calculated per 100,000 population per year; 95% confidence intervals (CI) were calculated for rate comparison. The direct method was used for age standardization. Proportions were compared using the chi-squared test at a p<0.05 significance level.
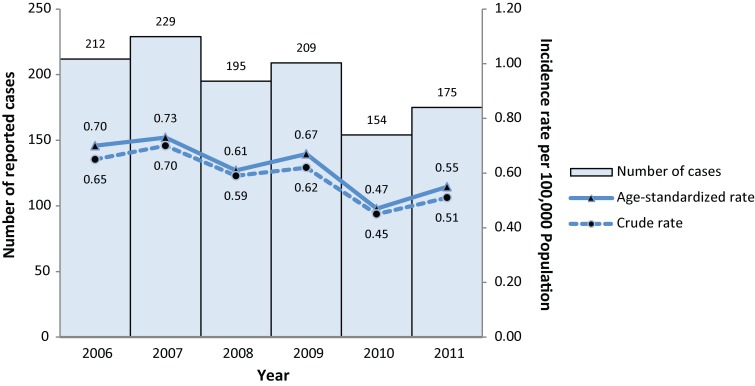
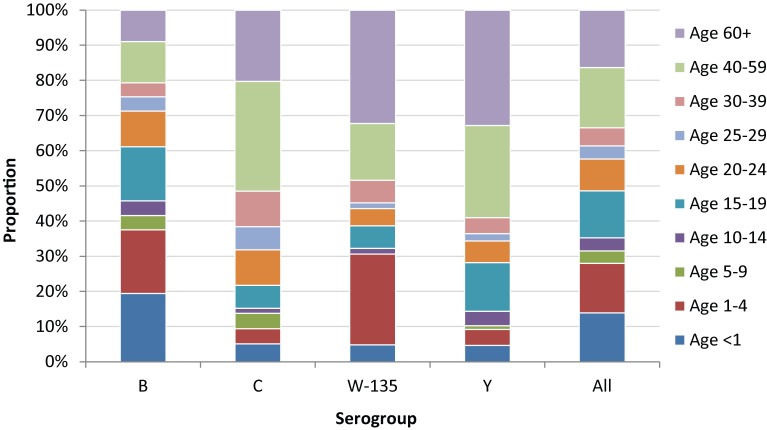
Results: During the study period, the mean incidence rates of IMD were 0.58 (total), 0.33 (serogroup B), 0.07 (serogroup C), 0.03 (serogroup W-135) and 0.10 (serogroup Y). The median age for serogroups B, C, W-135 and Y was 16, 43, 38 and 47 years respectively. The mean age-specific incidence rates among infants under 1 year of age (7.35, CI: 5.38-9.32) and children from 1 to 4 years of age (1.89, CI: 1.54-2.24) were significantly higher than those in any other age group. The mean case fatality ratio was 8.1% (range 4.3%-14.3%). The average number of cases that occurred per month was significantly higher (p<0.0001) in winter (18 cases) than in summer (12 cases).
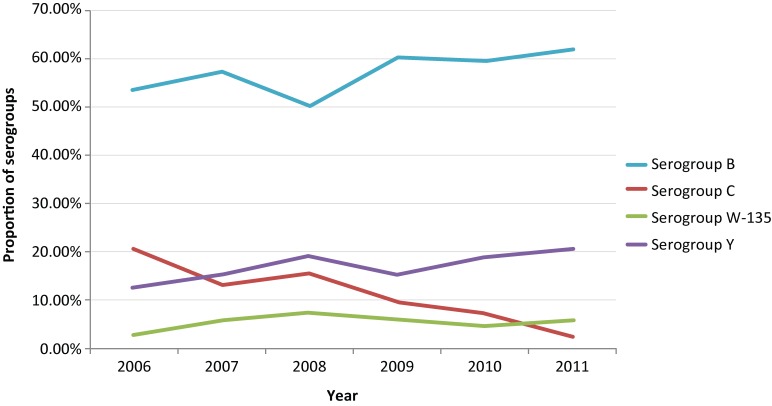
Conclusion: IMD is still endemic in Canada. Although individuals at any age can be affected, infants under 1 year of age are at the greatest risk, followed by children aged 1-4 years and individuals aged 15-19 years. Following the implementation of routine childhood immunization programs with monovalent meningococcal C conjugate vaccines (MenC) in all provinces and territories (beginning in 2007), the incidence of serogroup C has decreased significantly over the study period and is now at an all-time low. Serogroup B is the leading cause of IMD, and diseases of serogroup W-135 and Y have stabilized at relatively lower incidence rates. With the addition of immunization programs using quadrivalent conjugate meningococcal vaccines (MCV4), we would expect further reductions in the incidence of meningococcal infection in Canada.
Conflict of interest statement
Conflict of interest: No conflicts of interests to declare.
Figures

References
-
- Heymann DL. Control of Communicable Diseases Manual. 19th ed. American Public Health Association; 2008. p. 403.
-
- Mandell G, Bennett J, Dolin P. Chapter 211 – Neisseria meningitidis. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 7th ed. Philadelphia: Churchill Livingstone; 2009.
-
- Public Health Agency of Canada. Case definitions for communicable diseases under national surveillance. Can Commun Dis Rep 2009. Nov;35 Suppl 2.
-
- Varughese PV, Acres S. Meningococcal disease in Canada and serogroup distribution. Can Dis Wkly Rep 1983;9(45):177–80.
