

Regenerative medicine therapy for single ventricle congenital heart disease
- PMID: 29770299
- PMCID: PMC5938254
- DOI: 10.21037/tp.2018.04.01
Regenerative medicine therapy for single ventricle congenital heart disease
Abstract
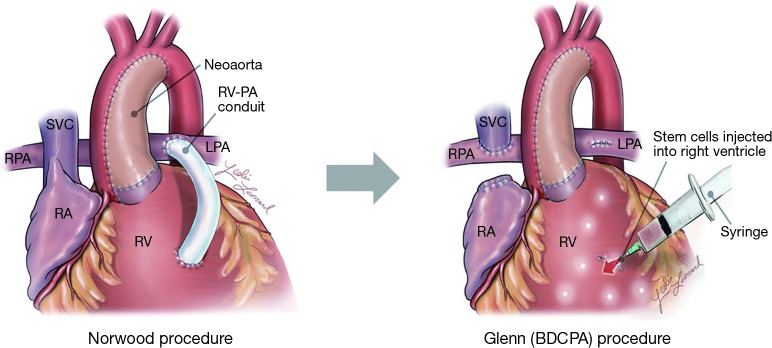
One of the most complex forms of congenital heart disease (CHD) involving single ventricle physiology is hypoplastic left heart syndrome (HLHS), characterized by underdevelopment of the left ventricle (LV), mitral and aortic valves, and narrowing of the ascending aorta. The underdeveloped LV is incapable of providing long-term systemic flow, and if left untreated, the condition is fatal. Current treatment for this condition consists of three consecutive staged palliative operations: the first is conducted within the first few weeks of birth, the second between 4 to 6 months, and the third and final surgery within the first 4 years. At the conclusion of the third surgery, systemic perfusion is provided by the right ventricle (RV), and deoxygenated blood flows passively to the pulmonary vasculature. Despite these palliative interventions, the RV, which is ill suited to provide long-term systemic perfusion, is prone to eventual failure. In the absence of satisfying curative treatments, stem cell therapy may represent one innovative approach to the management of RV dysfunction in HLHS patients. Several stem cell populations from different tissues (cardiac and non-cardiac), different age groups (adult- vs. neonate-derived), and different donors (autologous vs. allogeneic), are under active investigation. Preclinical trials in small and large animal models have elucidated several mechanisms by which these stem cells affect the injured myocardium, and are driving the shift from a paradigm based upon cellular engraftment and differentiation to one based primarily on paracrine effects. Recent studies have comprehensively evaluated the individual components of the stem cells' secretomes, shedding new light on the intracellular and extracellular pathways at the center of their therapeutic effects. This research has laid the groundwork for clinical application, and there are now several trials of stem cell therapies in pediatric populations that will provide important insights into the value of this therapeutic strategy in the management of HLHS and other forms of CHD. This article reviews the many stem cell types applied to CHD, their preclinical investigation and the mechanisms by which they might affect RV dysfunction in HLHS patients, and finally, the completed and ongoing clinical trials of stem cell therapy in patients with CHD.
Keywords: Heart defects; congenital; heart failure; hypoplastic left heart syndrome (HLHS); regenerative medicine; stem cells.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources