

Genetic Etiology for Alcohol-Induced Cardiac Toxicity
- PMID: 29773157
- PMCID: PMC5957753
- DOI: 10.1016/j.jacc.2018.03.462
Genetic Etiology for Alcohol-Induced Cardiac Toxicity
Abstract
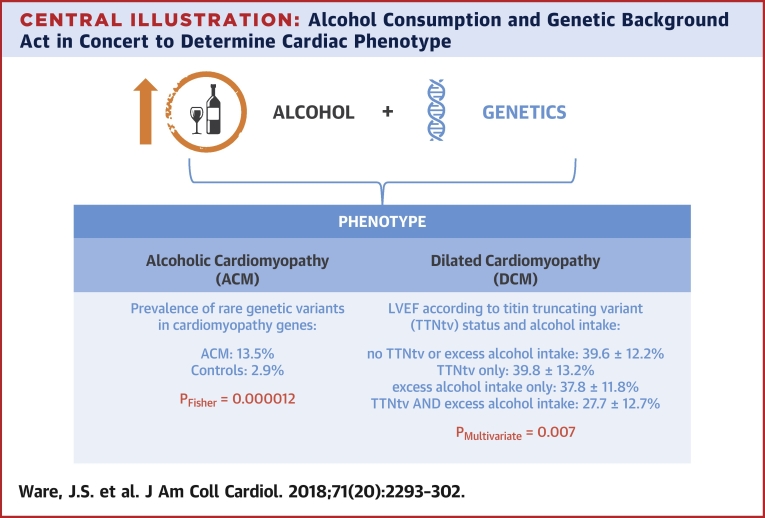
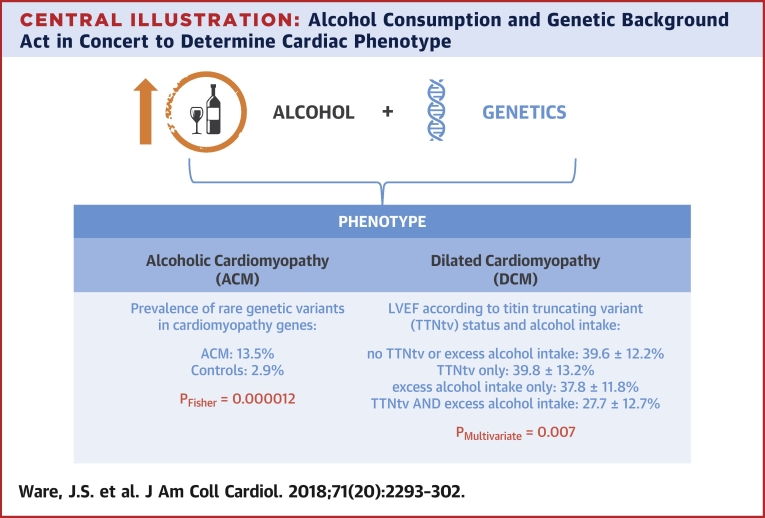
Background: Alcoholic cardiomyopathy (ACM) is defined by a dilated and impaired left ventricle due to chronic excess alcohol consumption. It is largely unknown which factors determine cardiac toxicity on exposure to alcohol.
Objectives: This study sought to evaluate the role of variation in cardiomyopathy-associated genes in the pathophysiology of ACM, and to examine the effects of alcohol intake and genotype on dilated cardiomyopathy (DCM) severity.
Methods: The authors characterized 141 ACM cases, 716 DCM cases, and 445 healthy volunteers. The authors compared the prevalence of rare, protein-altering variants in 9 genes associated with inherited DCM. They evaluated the effect of genotype and alcohol consumption on phenotype in DCM.
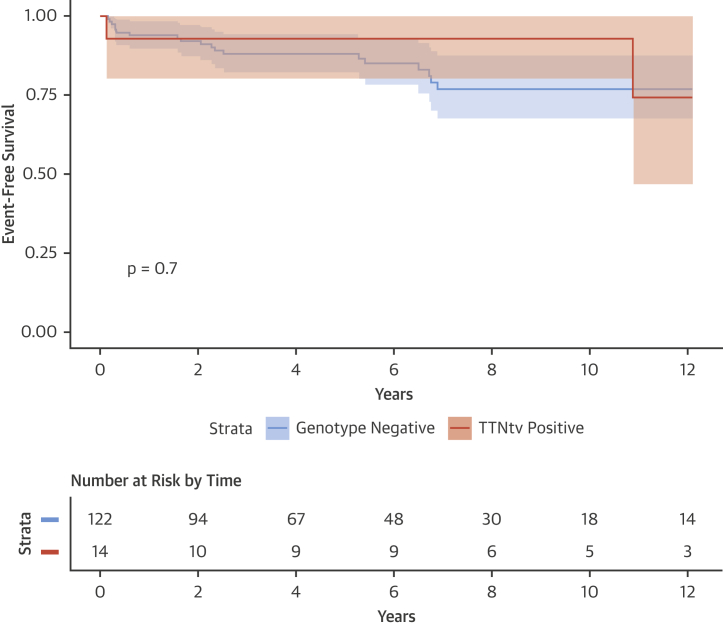
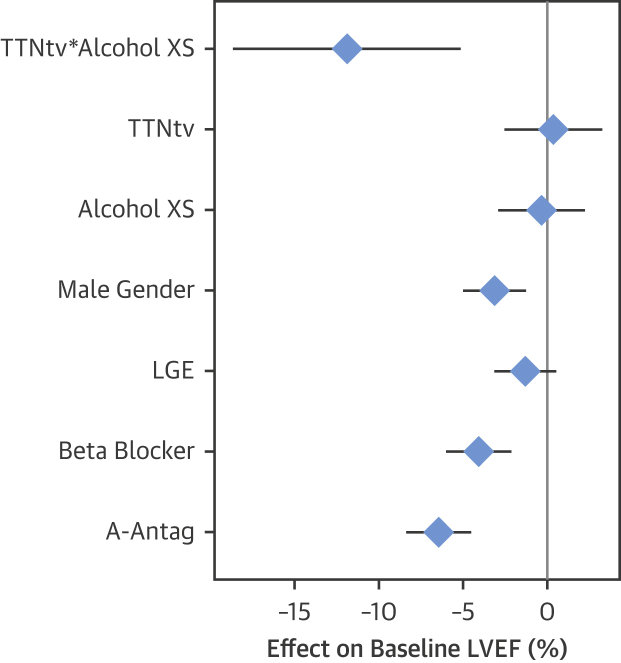
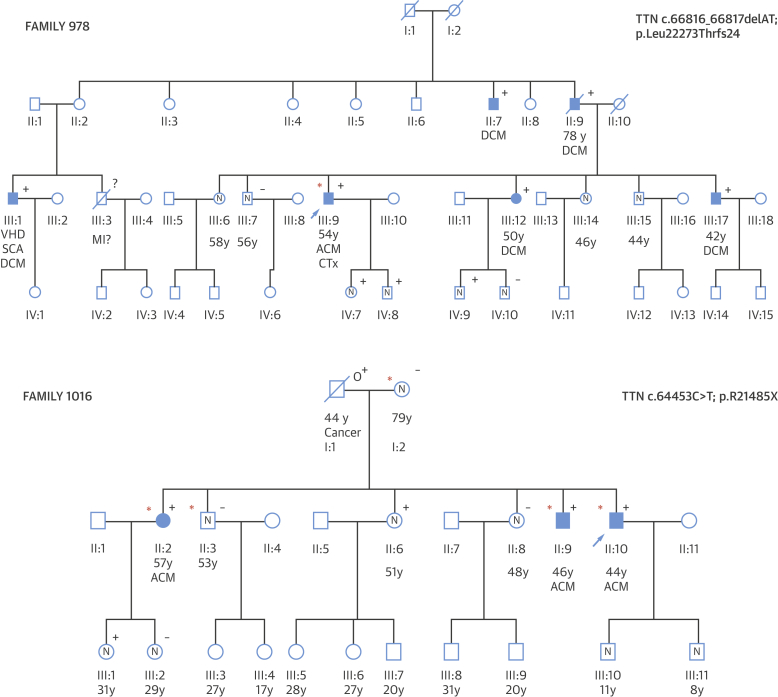
Results: Variants in well-characterized DCM-causing genes were more prevalent in patients with ACM than control subjects (13.5% vs. 2.9%; p = 1.2 ×10-5), but similar between patients with ACM and DCM (19.4%; p = 0.12) and with a predominant burden of titin truncating variants (TTNtv) (9.9%). Separately, we identified an interaction between TTN genotype and excess alcohol consumption in a cohort of DCM patients not meeting ACM criteria. On multivariate analysis, DCM patients with a TTNtv who consumed excess alcohol had an 8.7% absolute reduction in ejection fraction (95% confidence interval: -2.3% to -15.1%; p < 0.007) compared with those without TTNtv and excess alcohol consumption. The presence of TTNtv did not predict phenotype, outcome, or functional recovery on treatment in ACM patients.
Conclusions: TTNtv represent a prevalent genetic predisposition for ACM, and are also associated with a worse left ventricular ejection fraction in DCM patients who consume alcohol above recommended levels. Familial evaluation and genetic testing should be considered in patients presenting with ACM.
Keywords: alcohol; dilated cardiomyopathy; genetics; titin; variant.
Copyright © 2018 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Alcoholic Cardiomyopathy: Is it Time for Genetic Testing?J Am Coll Cardiol. 2018 May 22;71(20):2303-2305. doi: 10.1016/j.jacc.2018.03.463. J Am Coll Cardiol. 2018. PMID: 29773158 No abstract available.
References
-
- Urbano-Marquez A., Estruch R., Navarro-Lopez F., Grau J.M., Mont L., Rubin E. The effects of alcoholism on skeletal and cardiac muscle. N Engl J Med. 1989;320:409–415. - PubMed
-
- Fernandez-Sola J. Cardiovascular risks and benefits of moderate and heavy alcohol consumption. Nat Rev Cardiol. 2015;12:576–587. - PubMed
-
- Guzzo-Merello G., Segovia J., Dominguez F. Natural history and prognostic factors in alcoholic cardiomyopathy. J Am Coll Cardiol HF. 2015;3:78–86. - PubMed
-
- George A., Figueredo V.M. Alcoholic cardiomyopathy: a review. J Card Fail. 2011;17:844–849. - PubMed
-
- Xi B., Veeranki S.P., Zhao M., Ma C., Yan Y., Mi J. Relationship of alcohol consumption to all-cause, cardiovascular, and cancer-related mortality in U.S. adults. J Am Coll Cardiol. 2017;70:913–922. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
