

Medications received by patients with juvenile dermatomyositis
- PMID: 29773230
- PMCID: PMC6162169
- DOI: 10.1016/j.semarthrit.2018.03.016
Medications received by patients with juvenile dermatomyositis
Abstract
Objective: Few controlled studies are available to guide treatment decisions in juvenile dermatomyositis (JDM). This study evaluated therapies received, changes of treatment over time, and factors associated with medication choices in JDM.
Methods: We performed a retrospective analysis of the number and type of therapies and duration of treatment for 320 patients with JDM enrolled in a North American registry. Kaplan-Meier and logistic regression analysis were used to assess the association of demographic and clinical features and autoantibodies with medication usage.
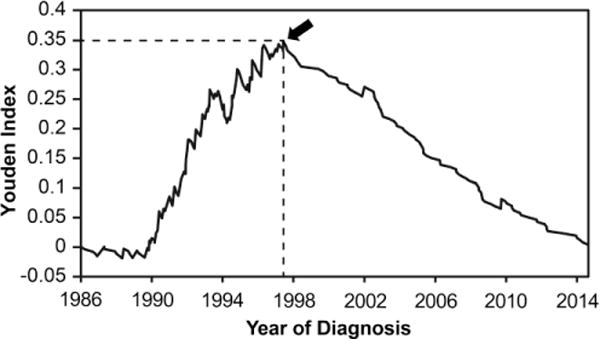
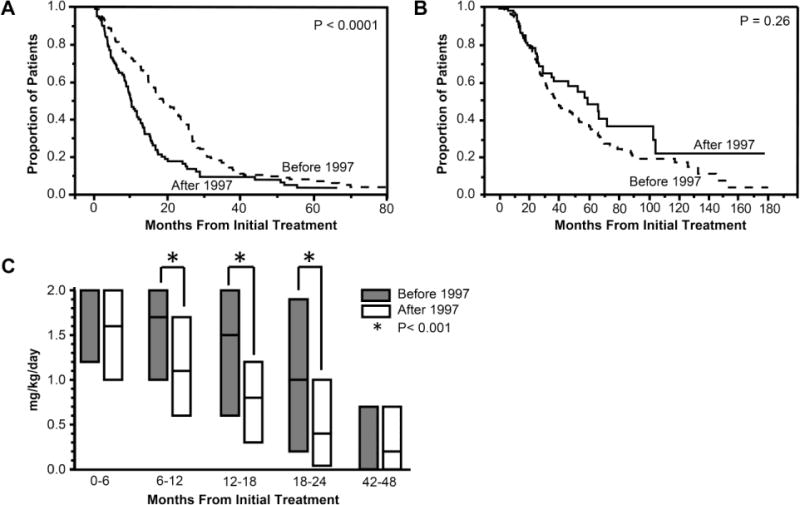
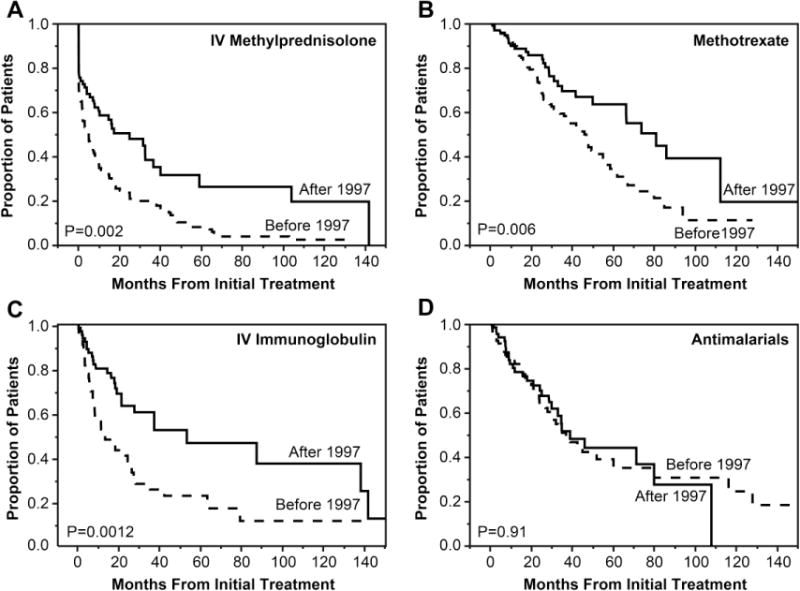
Results: High-dose oral prednisone was the primary therapy given to 99% of patients. 1997 was determined to be a threshold year for increasing usage of medications other than prednisone. The median time to half the initial oral prednisone dose was shorter in patients diagnosed after vs. before 1997 (10 vs. 19 months, P < 0.01). Patients received intravenous methylprednisolone (IVMP), methotrexate, intravenous immunoglobulin, antimalarial drugs, and combination therapy more frequently when diagnosed after 1997. IVMP was frequently received by patients with severe illness onset, anti-p155/140 (anti-TIF1) and anti-MJ (anti-NXP2) autoantibodies. Treatment with methotrexate was associated with older age at diagnosis and anti-MJ autoantibodies, while antimalarial therapy was associated with anti-p155/140 autoantibodies and mild onset severity.
Conclusion: Oral prednisone has been the mainstay of therapy in JDM, and prednisone was reduced faster in patients diagnosed after 1997 when there was also an increase in other medications. Specific medications received by patients with JDM correlated with year and age at diagnosis, myositis autoantibodies, onset severity, and illness features.
Keywords: Juvenile dermatomyositis; Medications; Methotrexate; Myositis autoantibodies; Prednisone; Treatment.
Published by Elsevier Inc.
Conflict of interest statement
Figures
References
-
- Feldman BM, Rider LG, Reed AM, Pachman LM. Juvenile dermatomyositis and other idiopathic inflammatory myopathies of childhood. Lancet. 2008;371:2201–12. - PubMed
-
- Bowyer SL, Blane CE, Sullivan DB, Cassidy JT. Childhood dermatomyositis: factors predicting functional outcome and development of dystrophic calcification. J Pediatr. 1983;103:882–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
