

Safety and efficacy of second-line bosutinib for chronic phase chronic myeloid leukemia over a five-year period: final results of a phase I/II study
- PMID: 29773593
- PMCID: PMC6068045
- DOI: 10.3324/haematol.2017.171249
Safety and efficacy of second-line bosutinib for chronic phase chronic myeloid leukemia over a five-year period: final results of a phase I/II study
Abstract
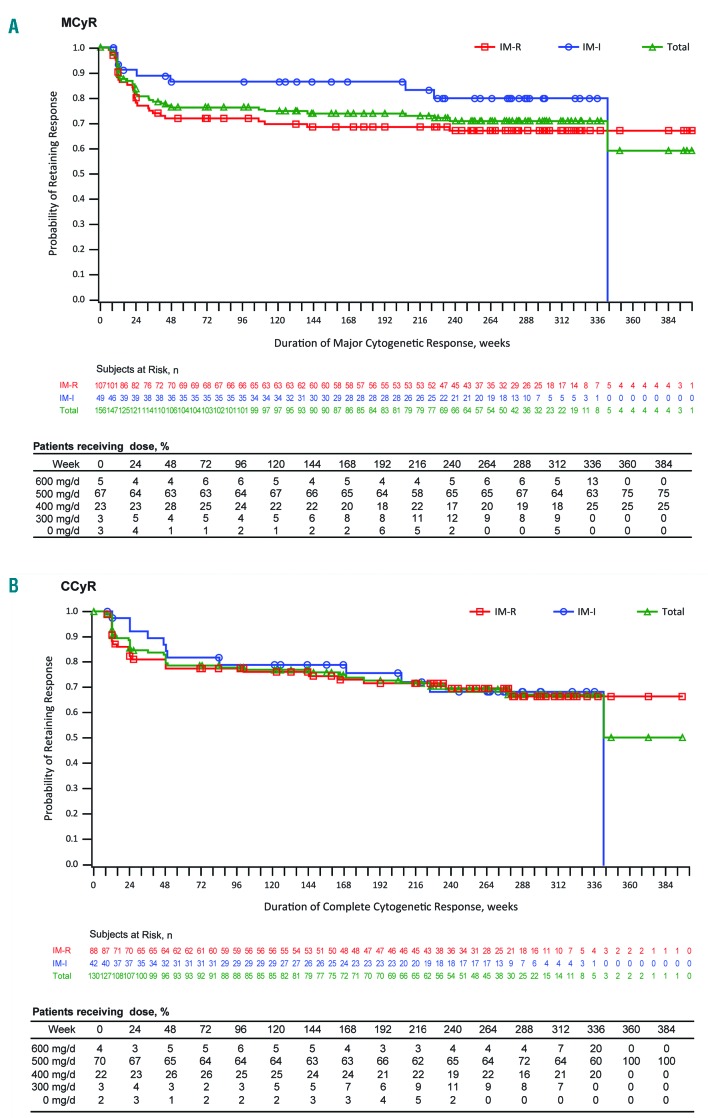
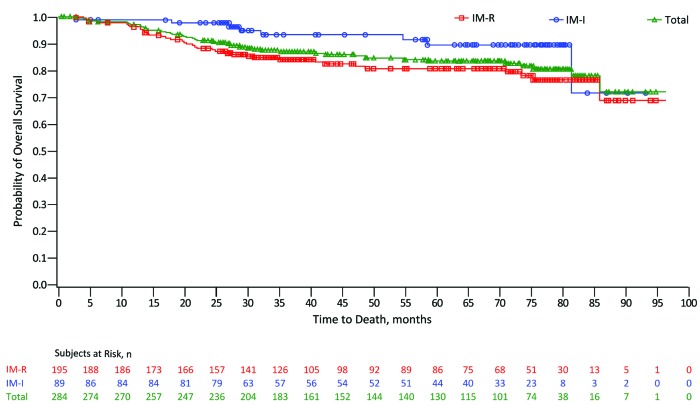
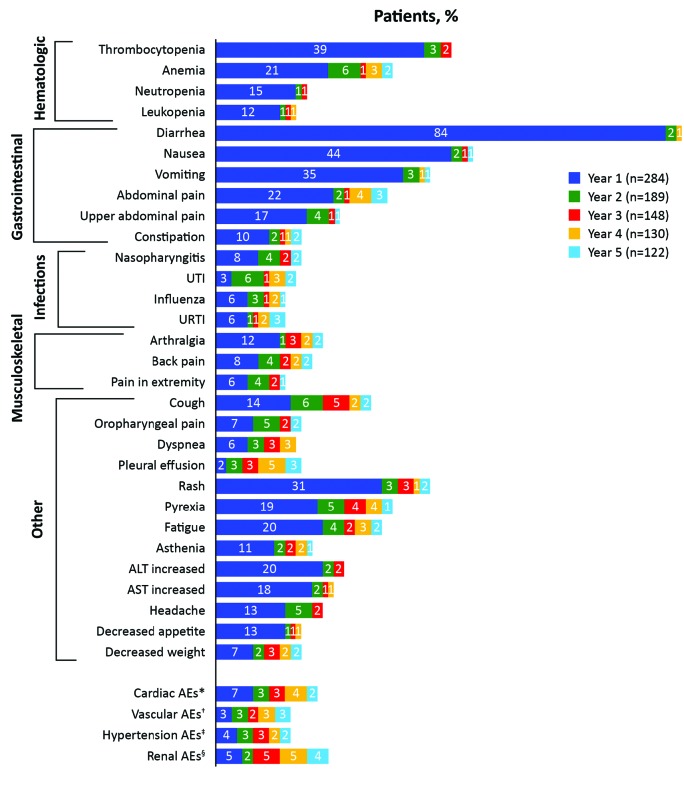
Bosutinib is a Src/Abl tyrosine kinase inhibitor indicated for adults with newly-diagnosed Philadelphia positive chronic myeloid leukemia or with resistant/intolerant disease. We report the final results of a phase I/II study of second-line bosutinib in chronic phase chronic myeloid leukemia patients after imatinib failure (n=284). Median follow up and treatment durations were 54.8 (range 0.6-96.3) and 25.6 (0.2-96.3) months, respectively. At years 2 and 5, 54% and 40% of patients, respectively, remained on bosutinib. Cumulative major cytogenetic response and complete cytogenetic response rates (newly-attained or maintained from baseline) were 58% and 46%, respectively, by year 2 and 60% and 50% by year 5. Kaplan-Meier probability of maintaining major and complete cytogenetic response was 76% and 78%, respectively, at year 2 and 71% and 69% at year 5. Cumulative incidence of on-treatment disease progression/death was similar at years 5 (19%) and 2 (15%); Kaplan-Meier overall survival was 91% at year 2 and 84% at year 5. Of 169 patients who had discontinued bosutinib by year 5, 38 did so after year 2, most commonly for disease progression (n=11). Most adverse events initially occurred within two years. Overall, gastrointestinal events were the most common (diarrhea 86%, nausea 46%, vomiting 37%); the most common grade 3/4 toxicity was thrombocytopenia (25%). None of the 4 on-treatment deaths in years 3-5 were related to bosutinib. Bosutinib demonstrated durable efficacy and manageable toxicity through year 5 confirming its importance in the treatment of chronic phase chronic myeloid leukemia patients resistant/intolerant to prior imatinib. This trial was registered at clinicaltrials.gov identifier: 00261846.
Trial registration: ClinicalTrials.gov NCT00261846.
Copyright© 2018 Ferrata Storti Foundation.
Figures
References
-
- Gambacorti-Passerini C, Antolini L, Mahon FX, et al. Multicenter independent assessment of outcomes in chronic myeloid leukemia patients treated with imatinib. J Natl Cancer Inst. 2011;103(7):553–561. - PubMed
-
- Vigano I, Di Giacomo N, Bozzani S, Antolini L, Piazza R, Gambacorti Passerini C. First-line treatment of 102 chronic myeloid leukemia patients with imatinib: a long-term single institution analysis. Am J Hematol. 2014;89(10):E184–187. - PubMed
-
- GLEEVEC® (imatinib mesylate). Full Prescribing Information. Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA, 2016.
-
- TASIGNA® (nilotinib). Full Prescribing Information. Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA, 2016.
-
- SPRYCEL® (dasatinib). Full Prescribing Information. Bristol-Myers Squibb Company, Princeton, NJ, USA, 2016.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
