

Unresolved endoplasmic reticulum stress engenders immune-resistant, latent pancreatic cancer metastases
- PMID: 29773669
- PMCID: PMC6547380
- DOI: 10.1126/science.aao4908
Unresolved endoplasmic reticulum stress engenders immune-resistant, latent pancreatic cancer metastases
Abstract
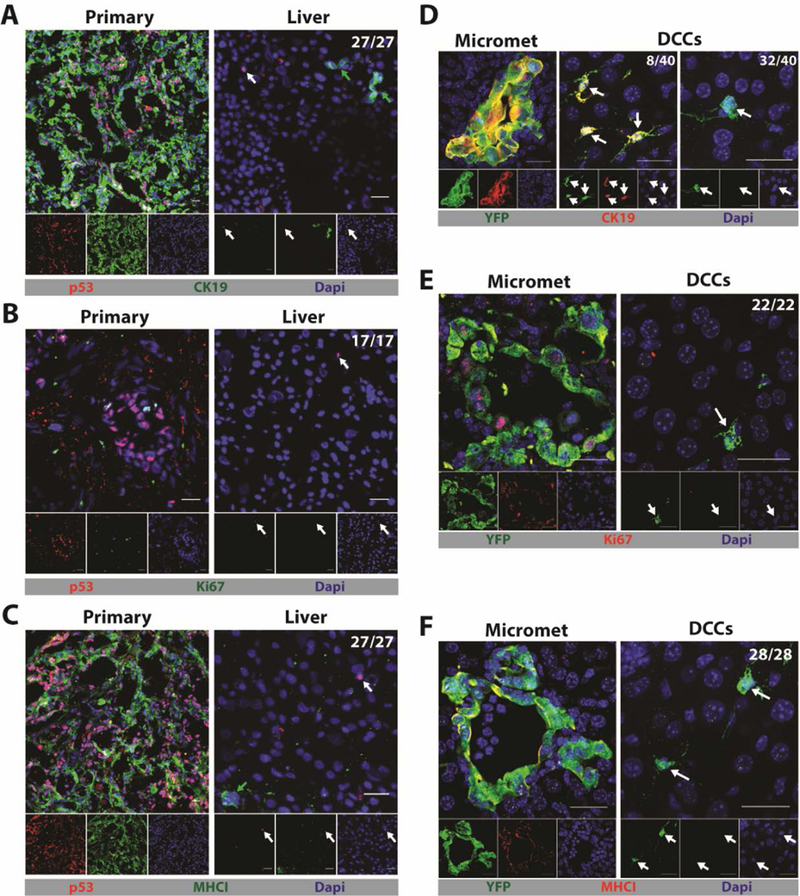
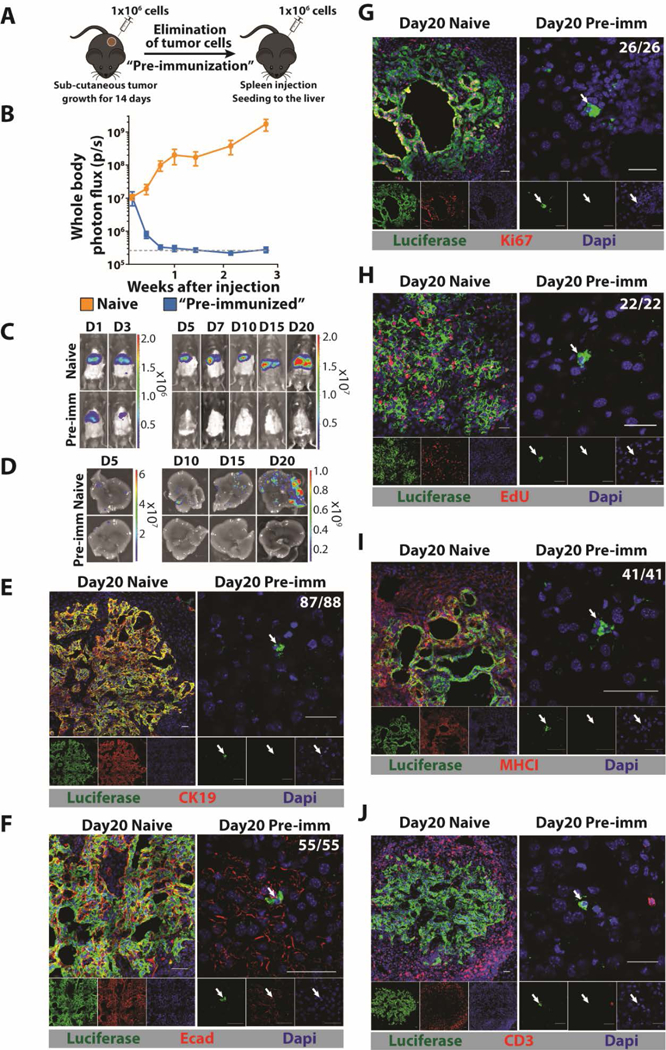
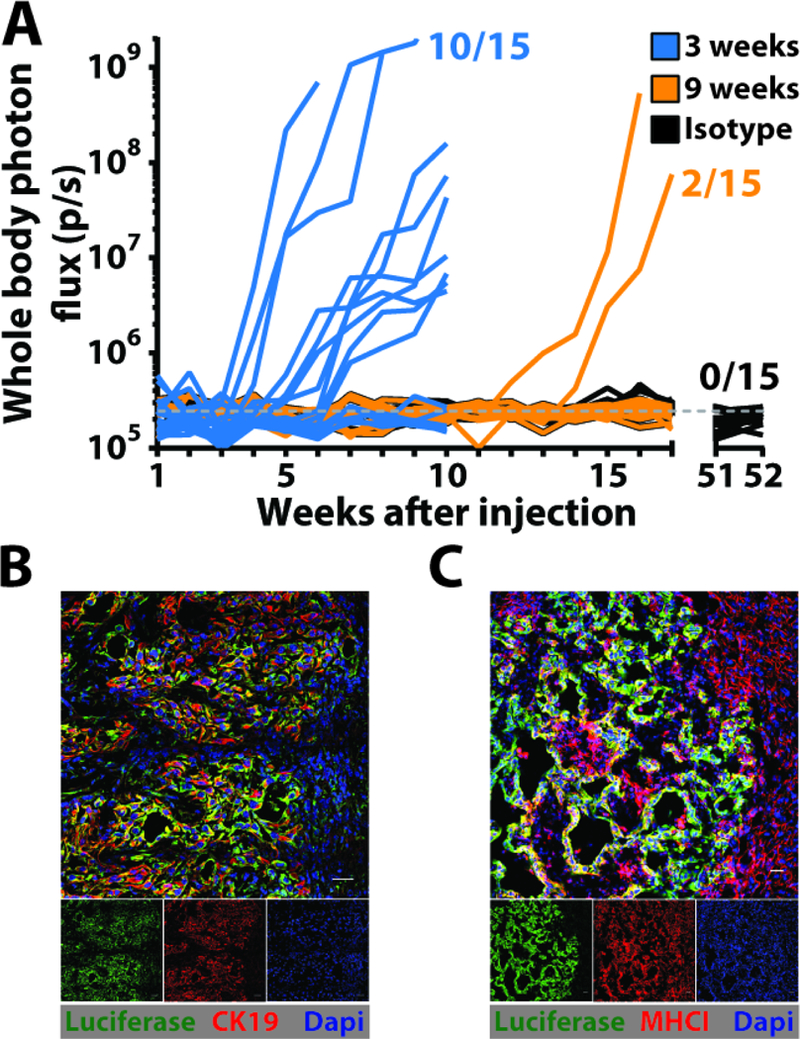
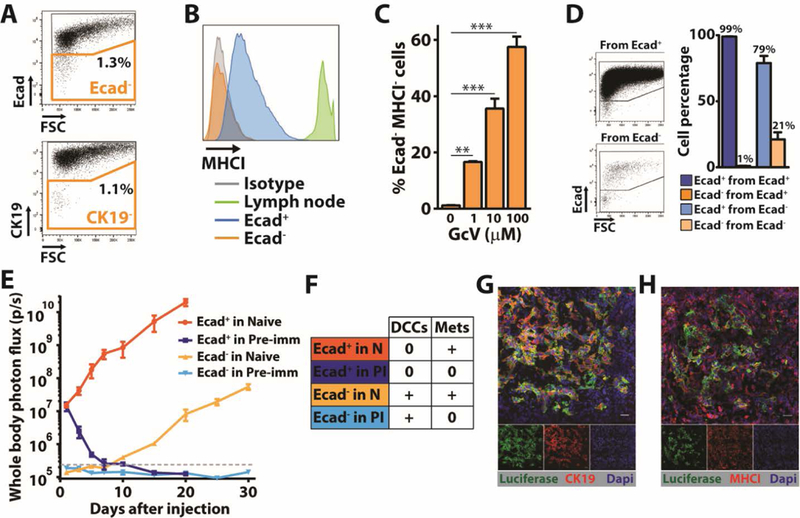
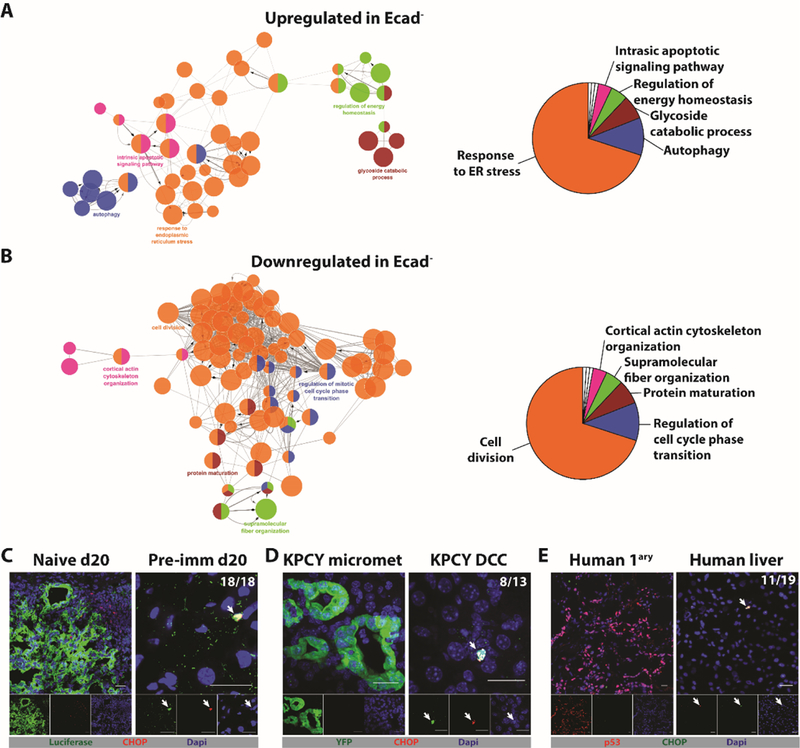
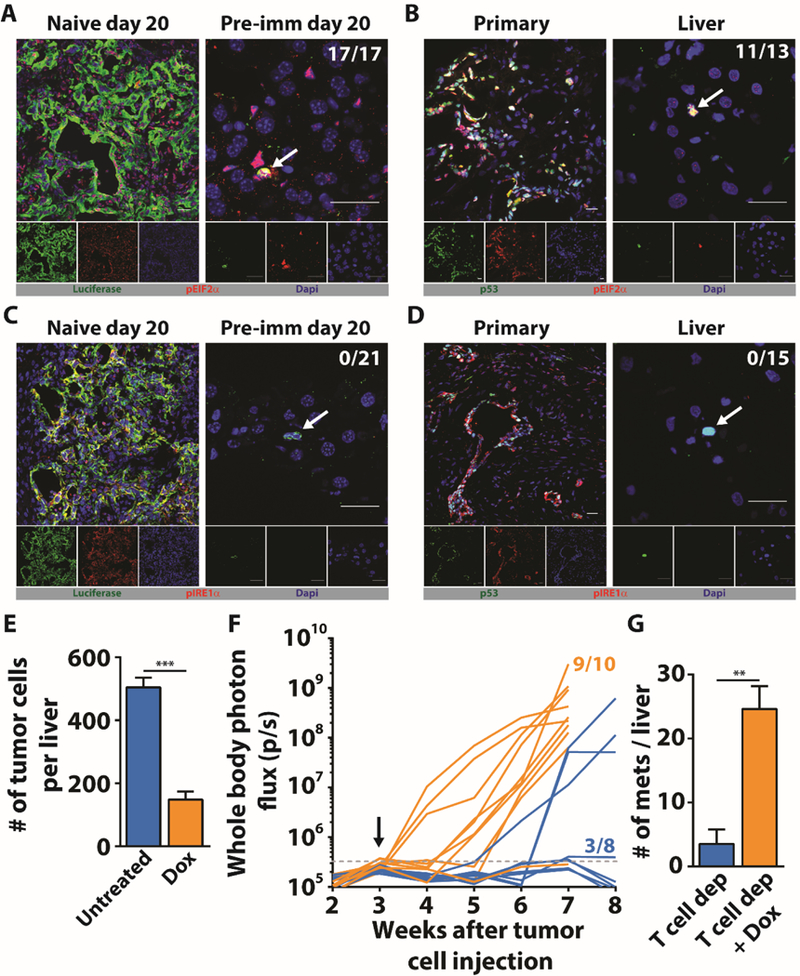
The majority of patients with pancreatic ductal adenocarcinoma (PDA) develop metastatic disease after resection of their primary tumor. We found that livers from patients and mice with PDA harbor single disseminated cancer cells (DCCs) lacking expression of cytokeratin 19 (CK19) and major histocompatibility complex class I (MHCI). We created a mouse model to determine how these DCCs develop. Intraportal injection of immunogenic PDA cells into preimmunized mice seeded livers only with single, nonreplicating DCCs that were CK19- and MHCI- The DCCs exhibited an endoplasmic reticulum (ER) stress response but paradoxically lacked both inositol-requiring enzyme 1α activation and expression of the spliced form of transcription factor XBP1 (XBP1s). Inducible expression of XBP1s in DCCs, in combination with T cell depletion, stimulated the outgrowth of macrometastatic lesions that expressed CK19 and MHCI. Thus, unresolved ER stress enables DCCs to escape immunity and establish latent metastases.
Copyright © 2018, American Association for the Advancement of Science.
Figures
Comment in
-
Balance of stresses guides metastasis.Nat Rev Gastroenterol Hepatol. 2018 Sep;15(9):520. doi: 10.1038/s41575-018-0047-0. Nat Rev Gastroenterol Hepatol. 2018. PMID: 29985452 No abstract available.
References
-
- Groot VP et al. , Patterns, Timing, and Predictors of Recurrence Following Pancreatectomy for Pancreatic Ductal Adenocarcinoma. Ann Surg, (March 23, 2017). - PubMed
-
- Van den Broeck A et al. , Patterns of recurrence after curative resection of pancreatic ductal adenocarcinoma. Eur J Surg Oncol 35, 600 (June, 2009). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
