

Diagnosis, Incidence, Predictors and Management of Postreperfusion Syndrome in Pediatric Deceased Donor Liver Transplantation: A Single-Center Study
- PMID: 29773782
- PMCID: PMC6248285
- DOI: 10.12659/AOT.909050
Diagnosis, Incidence, Predictors and Management of Postreperfusion Syndrome in Pediatric Deceased Donor Liver Transplantation: A Single-Center Study
Abstract
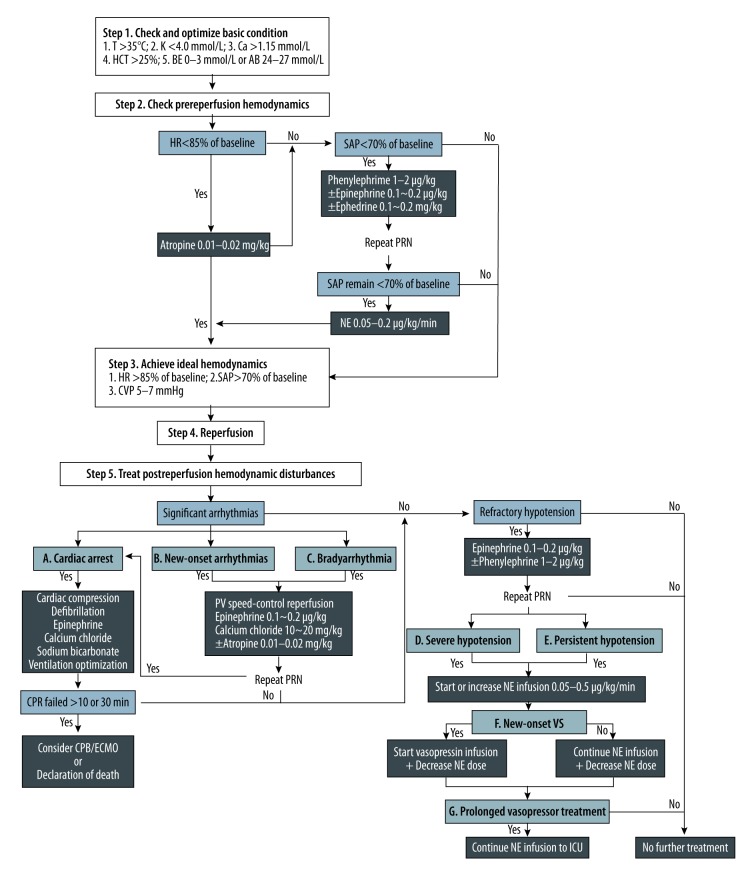
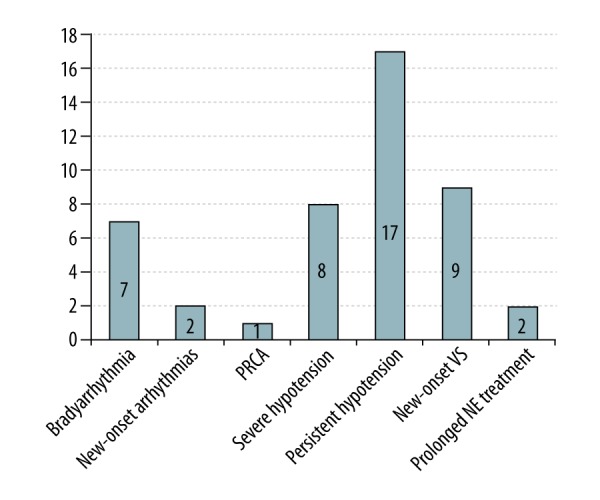
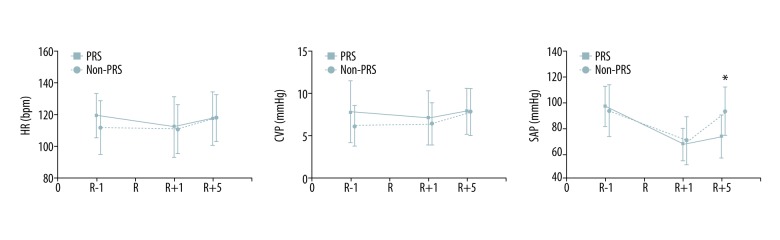
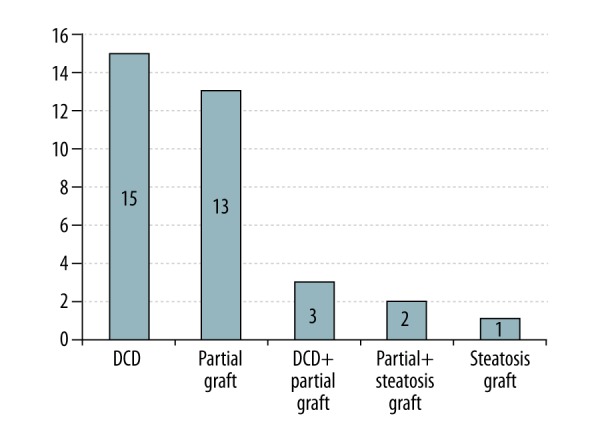
BACKGROUND Postreperfusion syndrome (PRS) is a dreadful and well-documented complication in adult liver transplantation (LT). However, information regarding PRS in pediatric LT is still scarce. We aimed to identify the incidence, risk factors and associated outcomes of pediatric LT in a single-center study. MATERIAL AND METHODS The medical records of 75 consecutive pediatric patients who underwent deceased donor liver transplantation (DDLT) from July 2015 to October 2017 were retrospectively reviewed. PRS was determined according to the Peking criteria when significant arrhythmia or refractory hypotension occurred following revascularization of the liver graft. Patients were divided into PRS and non-PRS groups. Preoperative, intraoperative, and postoperative data were collected and compared between the 2 groups. Independent risk factors for PRS were analyzed using binary logistic regression analysis. RESULTS PRS occurred in 26 patients (34.7%). Univariate analysis showed that the graft-to-recipient weight ratio (P=0.023), donor warm ischemia time (P<0.001), and the use of an expanded criteria donor (ECD) liver graft (P<0.001) were significant predictors of PRS. Binary logistic regression showed that the use of an ECD liver graft (odds ratio [OR]: 18.668; 95% confidence interval [95% CI]: 4.866-71.622) and lower hematocrit (HCT) level before reperfusion (OR: 0.878; 95% CI: 0.782-0.985) were independent predictors of PRS. PRS was significantly associated with early allograft dysfunction (73.1% vs. 18.4%, P<0.001), primary nonfunction (11.5% vs. 0.0%, P=0.039), and a prolonged hospital stay (median: 30.5 vs. 21.0, P=0.007). CONCLUSIONS The use of an ECD liver graft and lower HCT level before reperfusion were independent risk factors for PRS in pediatric DDLT. Intraoperative PRS occurrence seems to be associated with poor liver allograft function and worsened patient postoperative outcomes.
Conflict of interest statement
None.
Figures
References
-
- Daniela K, Michael Z, Florian I, et al. Influence of retrograde flushing via the caval vein on the post-reperfusion syndrome in liver transplantation. Clin Transplant. 2004;18(6):638–41. - PubMed
-
- Ryu HG, Jung CW, Lee CS, et al. Nafamostat mesilate attenuates postreperfusion syndrome during liver transplantation. Am J Transplant. 2011;11(5):977–83. - PubMed
-
- Bukowicka B, Akar RA, Olszewska A, et al. The occurrence of postreperfusion syndrome in orthotopic liver transplantation and its significance in terms of complications and short-term surval. Ann Transplant. 2011;16(2):26–30. - PubMed
-
- Hilmi I, Horton CN, Planinsic RM, et al. The impact of postreperfusion syndrome on short-term patient and liver allograft outcome in patients undergoing orthotopic liver transplantation. Liver Transpl. 2008;14(4):504–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
