

Cost-effectiveness of umeclidinium compared with tiotropium and glycopyrronium as monotherapy for chronic obstructive pulmonary disease: a UK perspective
- PMID: 29773969
- PMCID: PMC5946544
- DOI: 10.1186/s12962-018-0101-3
Cost-effectiveness of umeclidinium compared with tiotropium and glycopyrronium as monotherapy for chronic obstructive pulmonary disease: a UK perspective
Abstract
Background: Cost-effectiveness of once-daily umeclidinium bromide (UMEC) was compared with once-daily tiotropium (TIO) and once-daily glycopyrronium (GLY) in patients with chronic obstructive pulmonary disease (COPD) from a UK National Health Service (NHS) perspective.
Methods: A linked-equation model was implemented to estimate COPD progression, associated healthcare costs, exacerbations rates, life years (LY) and quality-adjusted LY (QALYs). Statistical risk equations for endpoints and resource use were derived from the ECLIPSE and TORCH studies, respectively. Treatment effects [mean (standard error)] at 12 weeks on forced expiratory volume in 1 s and St George's Respiratory Questionnaire score were obtained from the intention-to-treat populations of two head-to-head studies [GSK study identifiers 201316 (NCT02207829) and 201315 (NCT02236611)] which compared UMEC 62.5 mcg with TIO 18 mcg and UMEC 62.5 mcg with GLY 50 mcg, respectively. Treatment costs reflect UK list prices (2016) and NHS unit costs; UMEC and GLY prices being equal and less than TIO. A lifetime horizon, discounted costs and effects at 3.5% were used. Sensitivity analyses were performed to evaluate the robustness of variations in input parameters and assumptions in the model.
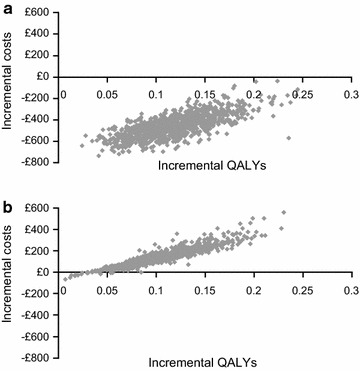
Results: Over a lifetime horizon, UMEC was predicted to increase LYs (+ 0.195; 95% confidence interval [CI]: 0.069, 0.356) and QALYs (+ 0.118; 95% CI: 0.055, 0.191) and reduce the number of annual exacerbations (- 0.053; 95% CI: - 0.171, 0.028) compared with TIO, with incremental cost savings of £460/patient (95% CI: - £645, - £240). Compared with GLY, UMEC increased LYs (+ 0.124; 95% CI: 0.015, 0.281) and QALYs (+ 0.101; 95% CI: 0.043, 0.179) and reduced annual exacerbation (- 0.033; 95% CI: - 0.135, 0.017) at an additional cost of £132/patient (95% CI: £12, £330), resulting in an incremental cost-effectiveness ratio of £1310/QALY (95% CI: £284, £2060). Similar results were observed in alternative time horizons and additional sensitivity analyses.
Conclusions: For treatment of patients with COPD in the UK over a lifetime horizon, treatment with UMEC dominates treatment with TIO, providing both improved health outcomes and cost savings. In comparison with GLY, treatment with UMEC achieved improved health outcomes but was associated with a higher cost.Trial registration 201316, NCT02207829; 201315, NCT02236611.
Keywords: Chronic obstructive pulmonary disorder; Cost-effectiveness; Economic evaluation; Long-acting muscarinic antagonist.
Figures
References
-
- Celli BR, Decramer M, Wedzicha JA, Wilson KC, Agusti AA, Criner GJ, MacNee W, Make BJ, Rennard SI, Stockley RA, et al. An official American Thoracic Society/European Respiratory Society statement: research questions in COPD. Eur Respir Rev. 2015;24:159–172. doi: 10.1183/16000617.00000315. - DOI - PMC - PubMed
-
- Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease. Updated 2017. http://goldcopd.org/gold-2017-global-strategy-diagnosis-management-preve.... Accessed 11 Apr 2017.
-
- GBD 2015 Chronic Respiratory Disease Collaborators Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2015;2017(5):691–706. - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
