

Different options of endosonography-guided biliary drainage after endoscopic retrograde cholangio-pancreatography failure
- PMID: 29774089
- PMCID: PMC5955728
- DOI: 10.4253/wjge.v10.i5.99
Different options of endosonography-guided biliary drainage after endoscopic retrograde cholangio-pancreatography failure
Abstract
Aim: To investigate the success rates of endosonography (EUS)-guided biliary drainage (EUS-BD) techniques after endoscopic retrograde cholangiopancreatography (ERCP) failure for management of biliary obstruction.
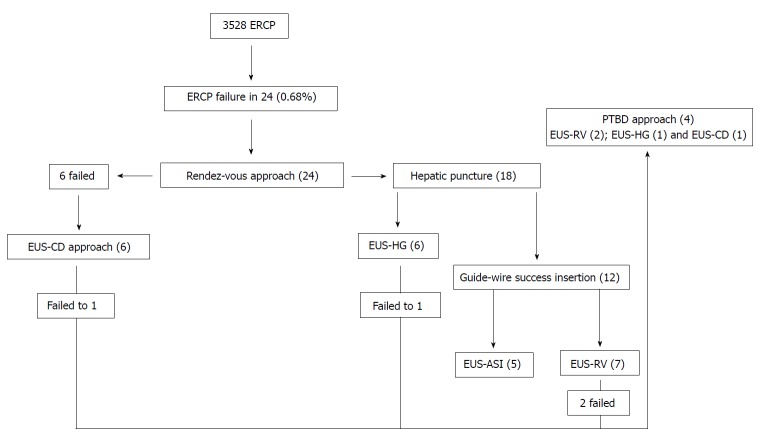
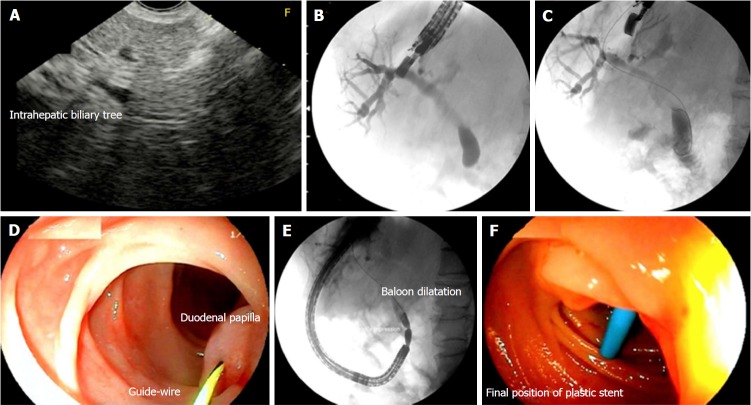
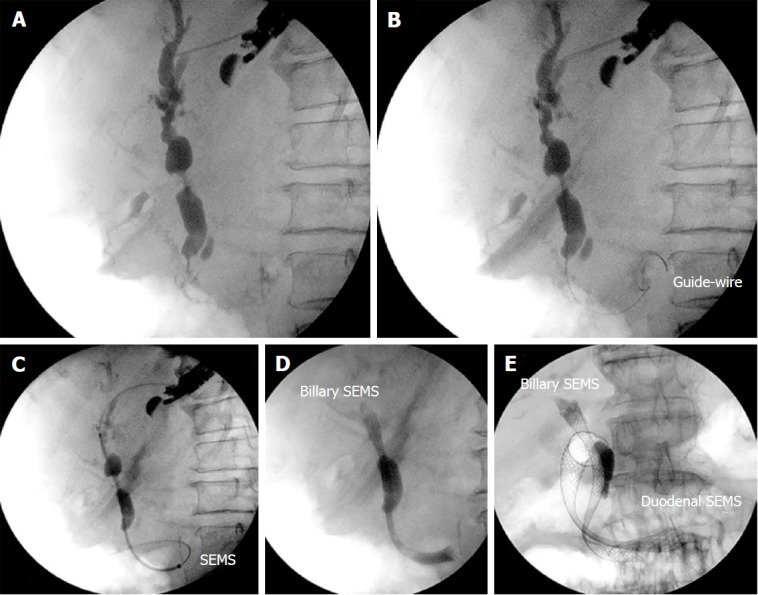
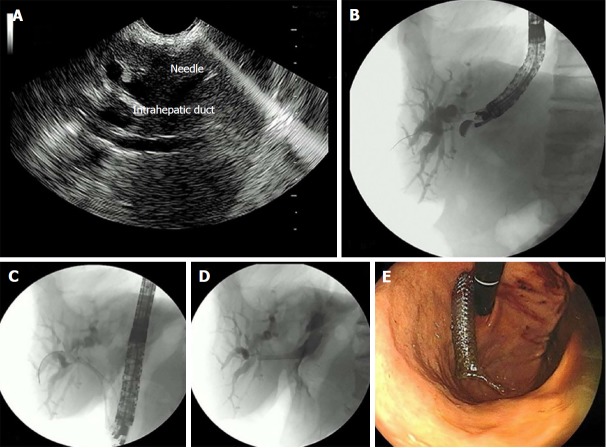
Methods: From Feb/2010 to Dec/2016, ERCP was performed in 3538 patients, 24 of whom (0.68%) suffered failure to cannulate the biliary tree. All of these patients were initially submitted to EUS-guided rendez-vous (EUS-RV) by means of a transhepatic approach. In case of failure, the next approach was an EUS-guided anterograde stent insertion (EUS-ASI) or an EUS-guided hepaticogastrostomy (EUS-HG). If a transhepatic approach was not possible or a guidewire could not be passed through the papilla, EUS-guided choledochoduodenostomy (EUS-CD) was performed.
Results: Patients were submitted to EUS-RV (7), EUS-ASI (5), EUS-HG (6), and EUS-CD (6). Success rates did not differ among the various EUS-BD techniques. Overall, technical and clinical success rates were 83.3% and 75%, respectively. Technical success for each technique was, 71.4%, 100%, 83.3%, and 83.3%, respectively (P = 0.81). Complications occurred in 3 (12.5%) patients. All of these cases were managed conservatively, but one patient died after rescue percutaneous transhepatic biliary drainage (PTBD).
Conclusion: The choice of a particular EUS-BD technique should be based on patient's anatomy and on whether the guidewire could be passed through the duodenal papilla.
Keywords: Cholestasis; Drainage; Endosonography; Interventional procedures; Jaundice; Neoplasms.
Conflict of interest statement
Conflict-of-interest statement: No potential conflicts of interest relevant to this article were reported.
Figures
References
-
- Carr-Locke DL. Overview of the role of ERCP in the management of diseases of the biliary tract and the pancreas. Gastrointest Endosc. 2002;56:S157–S160. - PubMed
-
- Fogel EL, Sherman S, Devereaux BM, Lehman GA. Therapeutic biliary endoscopy. Endoscopy. 2001;33:31–38. - PubMed
-
- Williams EJ, Ogollah R, Thomas P, Logan RF, Martin D, Wilkinson ML, Lombard M. What predicts failed cannulation and therapy at ERCP? Results of a large-scale multicenter analysis. Endoscopy. 2012;44:674–683. - PubMed
-
- Ferrucci JT Jr, Mueller PR, Harbin WP. Percutaneous transhepatic biliary drainage: technique, results, and applications. Radiology. 1980;135:1–13. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
