

An undifferentiated carcinoma at Klatskin-position with long-term complete remission after chemotherapy
- PMID: 29774134
- PMCID: PMC5955137
- DOI: 10.18632/oncotarget.25125
An undifferentiated carcinoma at Klatskin-position with long-term complete remission after chemotherapy
Abstract
Background: Neoplasms anatomically adjacent to the bile duct usually derive from malignantly transformed cholangiocytes forming cholangiocarcinoma (CCA). CCAs are divided in extrahepatic (eCCA) and intrahepatic (iCCA) tumors. Patients with irresectable CCAs are treated with systemic chemotherapy and have an unfavorable prognosis with a median survival of about one year. Here, we report a case of an undifferentiated carcinoma in Klatskin-position with long-term remission after systemic chemotherapy.
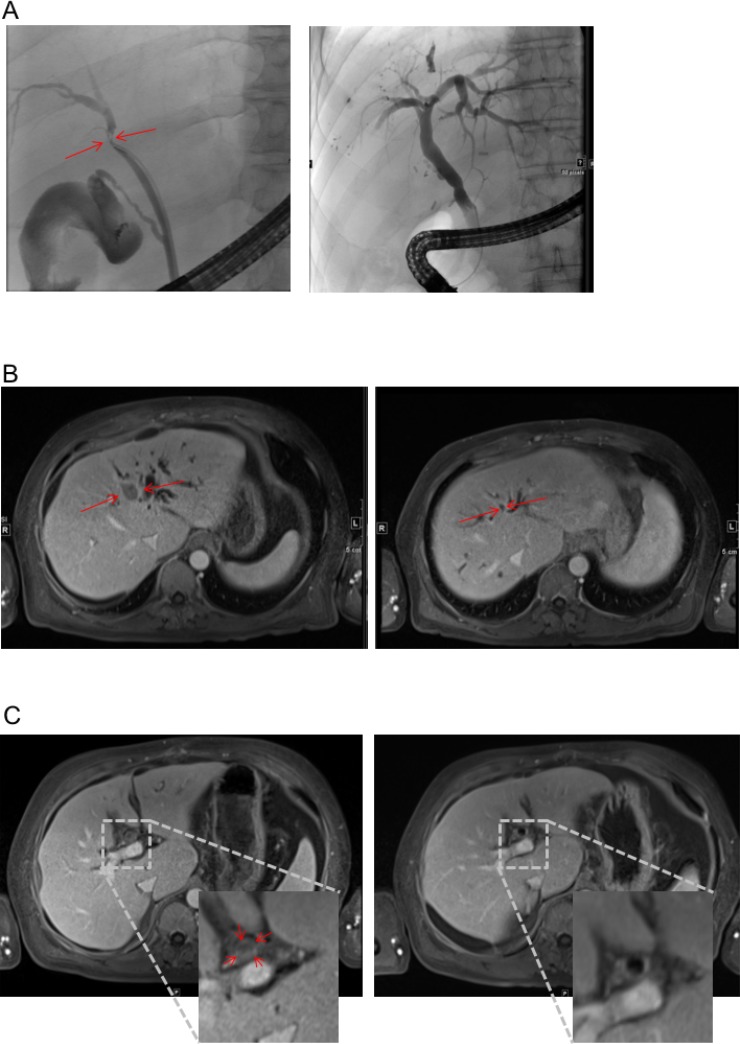
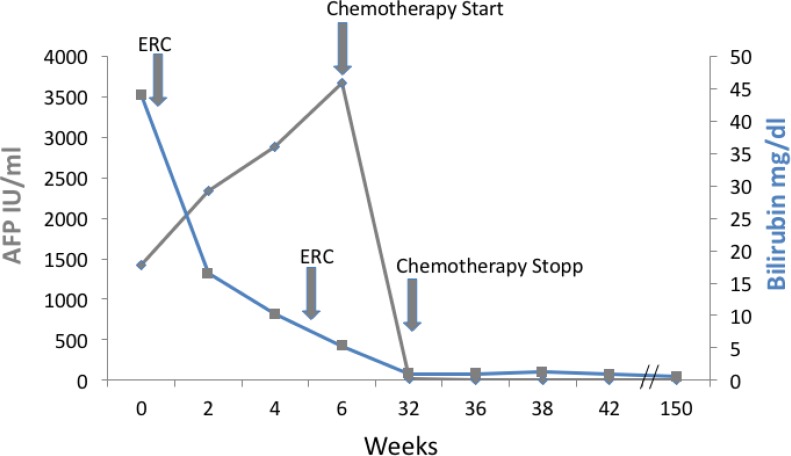
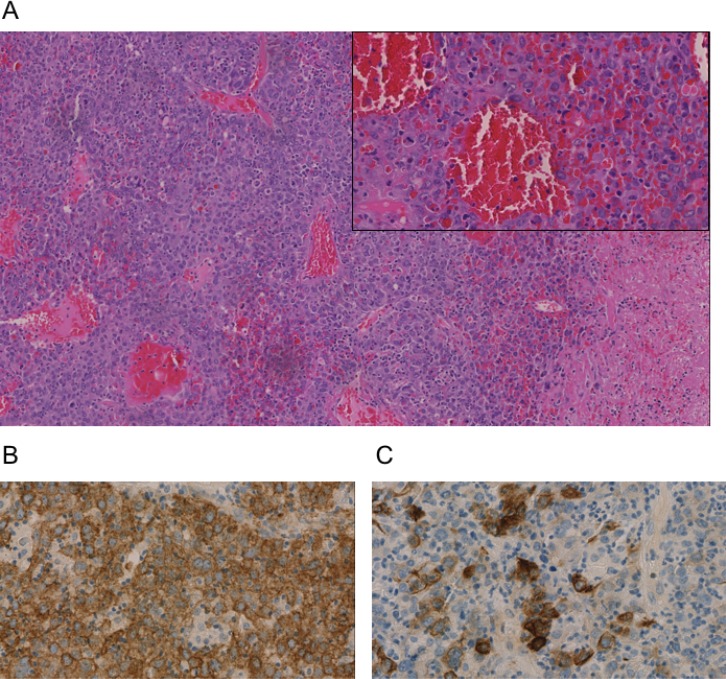
Case presentation: A 65-year-old Caucasian male presented with painless jaundice caused by an undifferentiated carcinoma in Klatskin-position (Type IIIb). Alpha fetoprotein (AFP; 3675 IU/mL) and carbohydrate antigen 19-9 (CA 19-9; 183 U/ml) were elevated. An exploratory laparotomy was carried out, but the patient was found to be irresectable due to severe fibrosis caused by biliary obstruction. Histology showed an undifferentiated carcinoma with high proliferation rate, and the patient was therefore subjected to poly-chemotherapy treatment according to the FOLFOX6-protocol. During therapy, AFP decreased to normal. Subsequent CT scans and ERC revealed a complete remission. Four years past initial diagnosis, a new suspicious lesion in the liver is visible on MRT; however, AFP and CA 19-9 are still in the normal range.
Conclusions: Our case demonstrates that histopathological defined diagnosis may significantly inform therapeutic decision-making in irresectable cholangiocarcinoma even in regard to conventional systemic therapy. In case of an undifferentiated carcinoma poly-chemotherapy may provide significant success.
Keywords: Klatskin tumor; chemotherapy; cholangiocarcinoma; endoscopic retrograde cholangiography; undifferentiated carcinoma.
Conflict of interest statement
CONFLICTS OF INTEREST None.
Figures
References
-
- Izbicki JR, Tsui TY, Bohn BA, Bockhorn M. Surgical strategies in patients with advanced hilar cholangiocarcinoma (Klatskin tumor) J Gastrointest Surg. 2013;17:581–5. - PubMed
-
- Singhal D, van Gulik TM, Gouma DJ. Palliative management of hilar cholangiocarcinoma. Surg Oncol. 2005;14:59–74. - PubMed
-
- Guro H, Kim JW, Choi Y, Cho JY, Yoon YS, Han HS. Multidisciplinary management of intrahepatic cholangiocarcinoma: Current approaches. Surg Oncol. 2017;26:146–152. - PubMed
-
- Liau JY, Tsai JH, Yuan RH, Chang CN, Lee HJ, Jeng YM. Morphological subclassification of intrahepatic cholangiocarcinoma: etiological, clinicopathological, and molecular features. Mod Pathol. 2014;27:1163–73. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
