

Pharmacokinetics and C-reactive protein modelling of anti-interleukin-6 antibody (PF-04236921) in healthy volunteers and patients with autoimmune disease
- PMID: 29776017
- PMCID: PMC6089821
- DOI: 10.1111/bcp.13641
Pharmacokinetics and C-reactive protein modelling of anti-interleukin-6 antibody (PF-04236921) in healthy volunteers and patients with autoimmune disease
Abstract
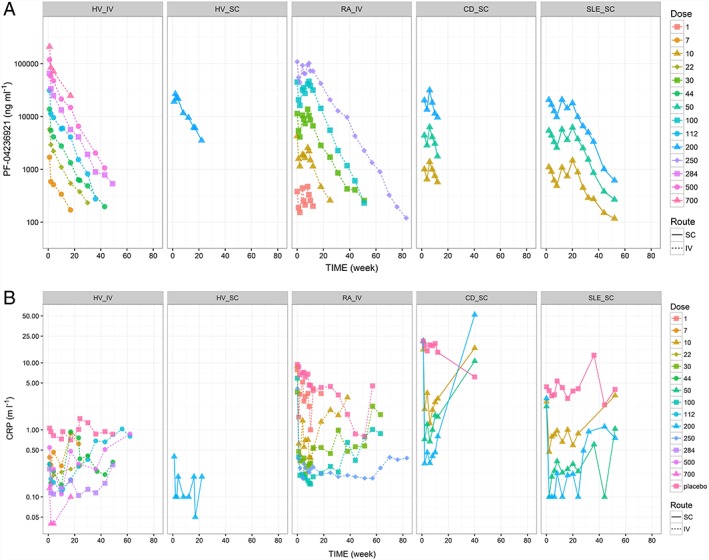
Aims: The purpose of this study was to characterize pharmacokinetics (PK) of PF-04236921, a novel anti-interleukin-6 monoclonal antibody, and its pharmacokinetic/pharmacodynamic (PK/PD) relationship on serum C-reactive protein (CRP) in healthy volunteers and patients with rheumatoid arthritis (RA), systemic lupus erythematosus (SLE) and Crohn's disease (CD).
Methods: Population modelling analyses were conducted using nonlinear mixed effects modelling. Data from two phase 1 healthy volunteer studies, a phase 1 RA study, a Phase 2 CD study and a Phase 2 SLE study were included.
Results: A two-compartment model with first order absorption and linear elimination and a mechanism-based indirect response model adequately described the PK and PK/PD relationships, respectively. Central compartment volume of distribution (Vc) positively correlated with body weight. Clearance (CL) negatively correlated with baseline albumin concentration and positively correlated with baseline CRP and creatinine clearance, and was slightly lower in females. After correcting for covariates, CL in CD subjects was approximately 60% higher than other populations. Maximum inhibition of PF-04236921 on CRP production (Imax ) negatively correlated with baseline albumin. Imax positively correlated with baseline CRP and the relationship was captured as a covariance structure in the PK/PD model.
Conclusion: Integrated population PK and PK/PD models of PF-04236921 have been developed using pooled data from healthy subjects and autoimmune patients. The current model enables simulation of PF-04236921 PK and PD profiles under various dosing regimens and patient populations and should facilitate future clinical study of PF-04236921 and other anti-interleukin-6 monoclonal antibodies.
Trial registration: ClinicalTrials.gov NCT00838565 NCT01287897 NCT01166555 NCT01405196.
Keywords: modelling and simulation; monoclonal antibodies; pharmacokinetic-pharmacodynamic; pharmacokinetics.
© 2018 The British Pharmacological Society.
Figures



References
-
- Catarzi S, Favilli F, Romagnoli C, Marcucci T, Picariello L, Tonelli F, et al Oxidative state and IL‐6 production in intestinal myofibroblasts of Crohn's disease patients. Inflamm Bowel Dis 2011; 17: 1674–1684. - PubMed
-
- Ito H. IL‐6 and Crohn's disease. Curr Drug Targets Inflamm Allergy 2003; 2: 125–130. - PubMed
-
- Tanaka T, Narazaki M, Kishimoto T. Anti‐interleukin‐6 receptor antibody, tocilizumab, for the treatment of autoimmune diseases. FEBS Lett 2011; 585: 3699–3709. - PubMed
-
- Fogel R, Sridharan S, Li C, Bradley J, Riese R, Labadie R, et al Safety, pharmacokinetics, and pharmacodynamics of a human anti‐IL6 monoclonal antibody PF‐04236921 in healthy subjects. Ann Rheum Dis 2013; 71 (Suppl 3): 680.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
