

MR-proADM as a Prognostic Marker in Patients With ST-Segment-Elevation Myocardial Infarction-DANAMI-3 (a Danish Study of Optimal Acute Treatment of Patients With STEMI) Substudy
- PMID: 29776961
- PMCID: PMC6015359
- DOI: 10.1161/JAHA.117.008123
MR-proADM as a Prognostic Marker in Patients With ST-Segment-Elevation Myocardial Infarction-DANAMI-3 (a Danish Study of Optimal Acute Treatment of Patients With STEMI) Substudy
Abstract
Background: Midregional proadrenomedullin (MR-proADM) has demonstrated prognostic potential after myocardial infarction (MI). Yet, the prognostic value of MR-proADM at admission has not been examined in patients with ST-segment-elevation MI (STEMI).
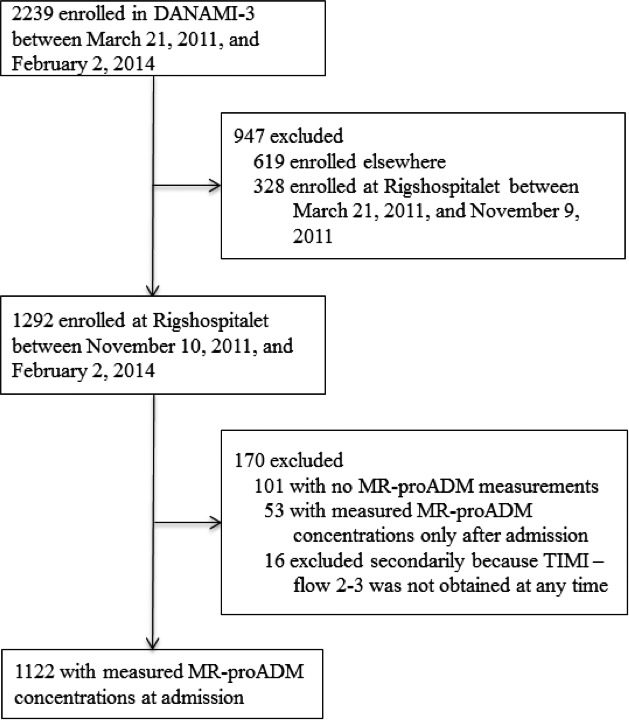
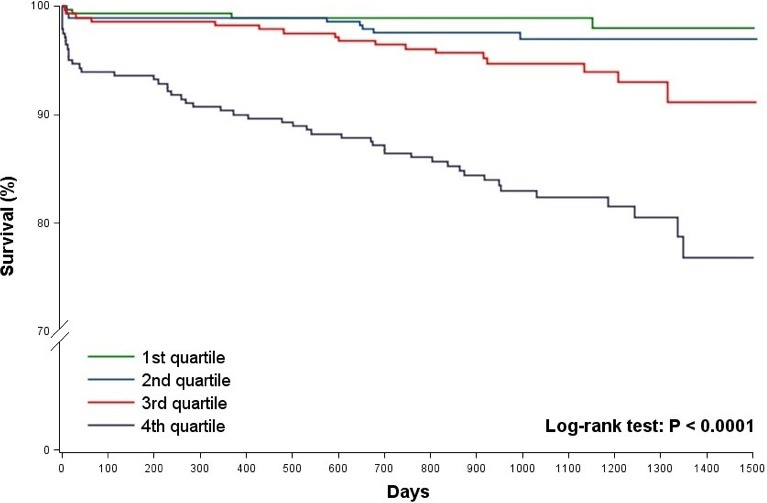
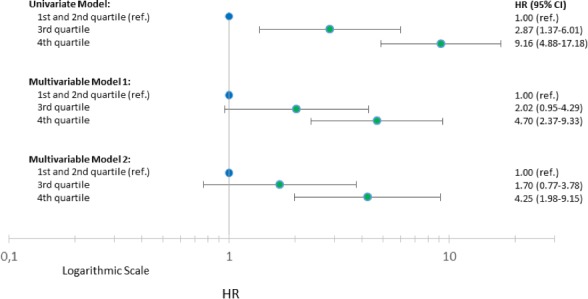
Methods and results: The aim of this substudy, DANAMI-3 (The Danish Study of Optimal Acute Treatment of Patients with ST-segment-elevation myocardial infarction), was to examine the associations of admission concentrations of MR-proADM with short- and long-term mortality and hospital admission for heart failure in patients with ST-segment-elevation myocardial infarction. Outcomes were assessed using Cox proportional hazard models and area under the curve using receiver operating characteristics. In total, 1122 patients were included. The median concentration of MR-proADM was 0.64 nmol/L (25th-75th percentiles, 0.53-0.79). Within 30 days 23 patients (2.0%) died and during a 3-year follow-up 80 (7.1%) died and 38 (3.4%) were admitted for heart failure. A doubling of MR-proADM was, in adjusted models, associated with an increased risk of 30-day mortality (hazard ratio, 2.67; 95% confidence interval, 1.01-7.11; P=0.049), long-term mortality (hazard ratio, 3.23; 95% confidence interval, 1.97-5.29; P<0.0001), and heart failure (hazard ratio, 2.71; 95% confidence interval, 1.32-5.58; P=0.007). For 30-day and 3-year mortality, the area under the curve for MR-proADM was 0.77 and 0.78, respectively. For 3-year mortality, area under the curve (0.84) of the adjusted model marginally changed (0.85; P=0.02) after addition of MR-proADM.
Conclusions: Elevation of admission MR-proADM was associated with long-term mortality and heart failure, whereas the association with short-term mortality was borderline significant. MR-proADM may be a marker of prognosis after ST-segment-elevation myocardial infarction but does not seem to add substantial prognostic information to established clinical models.
Clinical trial registration: URL: http:/www.ClinicalTrials.gov/. Unique identifiers: NCT01435408 and NCT01960933.
Keywords: ST‐segment–elevation myocardial infarction; biomarker; midregional proadrenomedullin; myocardial infarction; prognosis.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Similar articles
-
High Level of Mid-Regional Proadrenomedullin during ST-Segment Elevation Myocardial Infarction Is an Independent Predictor of Adverse Cardiac Events within 90-Day Follow-Up.Medicina (Kaunas). 2022 Jun 28;58(7):861. doi: 10.3390/medicina58070861. Medicina (Kaunas). 2022. PMID: 35888580 Free PMC article.
-
The prognostic value of neurohormonal and inflammatory biomarkers in addition to the TIMI risk score in patients with ST-elevation myocardial infarction.Biomarkers. 2025 Feb;30(1):1-9. doi: 10.1080/1354750X.2024.2435866. Epub 2025 Jan 7. Biomarkers. 2025. PMID: 39773138
-
Neurohormonal response is associated with mortality in women with ST-elevation myocardial infarction.Eur Heart J Acute Cardiovasc Care. 2025 Jan 31;14(1):31-39. doi: 10.1093/ehjacc/zuae141. Eur Heart J Acute Cardiovasc Care. 2025. PMID: 39657736
-
Predictive value of neutrophil to lymphocyte ratio in patients with acute ST segment elevation myocardial infarction after percutaneous coronary intervention: a meta-analysis.BMC Cardiovasc Disord. 2018 May 2;18(1):75. doi: 10.1186/s12872-018-0812-6. BMC Cardiovasc Disord. 2018. PMID: 29716535 Free PMC article. Review.
-
Prognostic value of neutrophil gelatinase-associated lipocalin in patients with acute ST-segment elevation myocardial infarction: A meta-analysis.Eur J Prev Cardiol. 2019 Mar;26(4):444-446. doi: 10.1177/2047487318783254. Epub 2018 Jun 19. Eur J Prev Cardiol. 2019. PMID: 29916725 No abstract available.
Cited by
-
Past, Present, and Future of Blood Biomarkers for the Diagnosis of Acute Myocardial Infarction-Promises and Challenges.Diagnostics (Basel). 2021 May 15;11(5):881. doi: 10.3390/diagnostics11050881. Diagnostics (Basel). 2021. PMID: 34063483 Free PMC article. Review.
-
Translational studies of adrenomedullin and related peptides regarding cardiovascular diseases.Hypertens Res. 2022 Mar;45(3):389-400. doi: 10.1038/s41440-021-00806-y. Epub 2022 Jan 6. Hypertens Res. 2022. PMID: 34992239 Free PMC article. Review.
-
High Level of Mid-Regional Proadrenomedullin during ST-Segment Elevation Myocardial Infarction Is an Independent Predictor of Adverse Cardiac Events within 90-Day Follow-Up.Medicina (Kaunas). 2022 Jun 28;58(7):861. doi: 10.3390/medicina58070861. Medicina (Kaunas). 2022. PMID: 35888580 Free PMC article.
-
Emerging Biomarkers for Predicting Clinical Outcomes in Patients with Heart Disease.Life (Basel). 2023 Jan 13;13(1):230. doi: 10.3390/life13010230. Life (Basel). 2023. PMID: 36676179 Free PMC article. Review.
-
Clinical Potential of Adrenomedullin Signaling in the Cardiovascular System.Circ Res. 2023 Apr 28;132(9):1185-1202. doi: 10.1161/CIRCRESAHA.123.321673. Epub 2023 Apr 27. Circ Res. 2023. PMID: 37104556 Free PMC article. Review.
References
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli‐Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, Hindricks G, Kastrati A, Lenzen MJ, Prescott E, Roffi M, Valgimigli M, Varenhorst C, Vranckx P, Widimsky P. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST‐segment elevation. Rev Esp Cardiol (Engl ed). 2017;70:1082. - PubMed
-
- Boersma E. Does time matter? A pooled analysis of randomized clinical trials comparing primary percutaneous coronary intervention and in‐hospital fibrinolysis in acute myocardial infarction patients. Eur Heart J. 2006;27:779–788. - PubMed
-
- Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361:13–20. - PubMed
-
- Kristensen SD, Laut KG, Fajadet J, Kaifoszova Z, Kala P, Di Mario C, Wijns W, Clemmensen P, Agladze V, Antoniades L, Alhabib KF, De Boer MJ, Claeys MJ, Deleanu D, Dudek D, Erglis A, Gilard M, Goktekin O, Guagliumi G, Gudnason T, Hansen KW, Huber K, James S, Janota T, Jennings S, Kajander O, Kanakakis J, Karamfiloff KK, Kedev S, Kornowski R, Ludman PF, Merkely B, Milicic D, Najafov R, Nicolini FA, Noc M, Ostojic M, Pereira H, Radovanovic D, Sabate M, Sobhy M, Sokolov M, Studencan M, Terzic I, Wahler S, Widimsky P. Reperfusion therapy for ST elevation acute myocardial infarction 2010/2011: current status in 37 ESC countries. Eur Heart J. 2014;35:1957–1970. - PubMed
-
- Pedersen F, Butrymovich V, Kelbaek H, Wachtell K, Helqvist S, Kastrup J, Holmvang L, Clemmensen P, Engstrom T, Grande P, Saunamaki K, Jorgensen E. Short‐ and long‐term cause of death in patients treated with primary PCI for STEMI. J Am Coll Cardiol. 2014;64:2101–2108. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
